It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Canadian doctor makes anti-Obamacare senator look like a buffoon
page: 1share:
www.salon.com...
America’s shame, through doctrinal narrow minded selfishness by mostly southern and western GOP politicians, while being a modern state where thousands die every year due to no health insurance, is laid bare by this exchange.
Typical GOP distortion to hide the ugly truth that America is the ONLY modern country in the world that doesn’t provide health care for ALL of its citizens.
The GOPer is as usual distorting facts to back up his inhuman philosophy, is corrected again.
Speaking before a Senate subcommittee on Tuesday, Dr. Danielle Martin, vice president at the Women’s College Hospital in Toronto, masterfully showed how to smack down a disingenuous politician’s misleading and misinformed questions with courtesy, intelligence and, well, facts.
In this instance, the role of disingenuous and ill-informed politician was played by North Carolina’s GOP Sen. Richard Burr, who decided to use his question time to imply that the Canadian healthcare system was bad because it led to Canadian doctors moving to America and rich people going to the U.S. to get complicated and expensive surgery. These were both good points — except for the fact that they were, as Martin made clear, completely wrong.
America’s shame, through doctrinal narrow minded selfishness by mostly southern and western GOP politicians, while being a modern state where thousands die every year due to no health insurance, is laid bare by this exchange.
“Dr. Martin, in your testimony, you note that Canadian doctors exiting the public system for the private sector has had the effect of increasing waiting lists for patients seeking public health care,” Burr began. “Why are doctors exiting the public system in Canada?”
Typical GOP distortion to hide the ugly truth that America is the ONLY modern country in the world that doesn’t provide health care for ALL of its citizens.
“Thank you for your question, Senator,” Martin responded. “If I didn’t express myself in a way that made myself understood, I apologize. There are no doctors exiting the public system in Canada; and in fact we see a net influx of physicians from the United States into the Canadian system over the last number of years.”
Martin then tried to reiterate her earlier point (which Burr had gotten about 100 percent wrong) by noting that “the solution to the wait-time challenge that we have in Canada … does not lie in moving away from our single-payer system to a multi-payer system.” She cited the Australian example, where the move from a single-payer to a multi-payer model actually led to wait times increasing.
Burr had no response to Martin’s corrections, however, and swiftly moved on to his next question. This, too, was premised on a well-worn anti-Obamacare GOP talking point, which also happened to be pretty wrong.
“What do you say to an elected official who goes to Florida and not the Canadian system to have a heart valve replaced?” Burr asked. “It’s actually interesting,” Martin responded, “because, in fact, the people who are the pioneers of that particular surgery … and have the best health outcomes in the world for that surgery, are in Toronto, at the Peter Munk Cardiac Center, just down the street from where I work.ext
The GOPer is as usual distorting facts to back up his inhuman philosophy, is corrected again.
“So what I say is that sometimes people have a perception — and I believe that actually this is fueled in part by media discourse — that going to where you pay more for something, that that necessarily makes it better, but it’s not actually borne out by the evidence on outcomes from that cardiac surgery or any other,” she added. Burr didn’t agree and went on to claim, referencing no evidence, that the reason Americans prefer their system is “because they judge quality and they judge innovation.” For what it’s worth, a 2013 study of how people in 11 countries felt about their healthcare system found about six in 10 U.K. citizens saying the NHS (which is similar to Canada’s Medicare) “works pretty well, and only minor changes are necessary to make it work better.” The number of Americans willing to say the same? About 29 percent
reply to post by Willtell
Did he seriously ask why Canadians don't want the same healthcare as Americans?
perhaps I misheard... but that's the silliest question I've ever heard
Did he seriously ask why Canadians don't want the same healthcare as Americans?
perhaps I misheard... but that's the silliest question I've ever heard
reply to post by Willtell
Ms. Pipes is clearly being a tool for someone, I think if we checked her finances we would find a conflict of interests somewhere. It is obvious for her participation what she is backing there (not really providing clarification but promoting the disinformation at every opportunity).
Ms. Pipes is clearly being a tool for someone, I think if we checked her finances we would find a conflict of interests somewhere. It is obvious for her participation what she is backing there (not really providing clarification but promoting the disinformation at every opportunity).
While I consider myself to be anti-Obamacare, whaat people need to understand is that being against the current Obamacare implementation doesn't mean
that we all believe the GOP claims either. For some of us, the coverage just isn't worth the money.
Coverage under Obamacare for myself and my spouse would run approx $850 a mo ($10,200 a yr), and require a $10,000 a year deductible. That's insane.
In our case, we would pay $10,000 a year just for the privilege to be covered, then would have to pay the first $10k out of pocket to meet the ANNUAL deductible before we even see any benefit. That's over $20,000! In my 50 years on this earh, I've never accumulated near that amount in medical related expenses, including the costs of having two kids. To expect me to hand that over every year is beyond highway robbery. If a person were to instead put $20k a year into an unlimited, tax-free health savings account, over the course of my 50 year working career I'd have put away over $1 mil to be used for my health needs, not including accrued intrest. How can anyone say that short of a catastrophic injury or illness, giving money to an insurance company is a better deal?
Keep your insurance. I'll invest mine as I see fit.
Coverage under Obamacare for myself and my spouse would run approx $850 a mo ($10,200 a yr), and require a $10,000 a year deductible. That's insane.
In our case, we would pay $10,000 a year just for the privilege to be covered, then would have to pay the first $10k out of pocket to meet the ANNUAL deductible before we even see any benefit. That's over $20,000! In my 50 years on this earh, I've never accumulated near that amount in medical related expenses, including the costs of having two kids. To expect me to hand that over every year is beyond highway robbery. If a person were to instead put $20k a year into an unlimited, tax-free health savings account, over the course of my 50 year working career I'd have put away over $1 mil to be used for my health needs, not including accrued intrest. How can anyone say that short of a catastrophic injury or illness, giving money to an insurance company is a better deal?
Keep your insurance. I'll invest mine as I see fit.
We Canadians love our health care system, despite its annoyances sometimes. What we absolutely hate are the extortionist parking rates in hospital
lots.
reply to post by Willtell
I recently signed up on the exchange and must say it has improved drastically from last year. I am an independent leaning toward libertarian, but i gave it a chance and yes 90 percent of what the GOP says is disinformation gathered from my personal experience. In fact the plan i got was with a popular insurance company.
I recently signed up on the exchange and must say it has improved drastically from last year. I am an independent leaning toward libertarian, but i gave it a chance and yes 90 percent of what the GOP says is disinformation gathered from my personal experience. In fact the plan i got was with a popular insurance company.
The end part of the video shows a better bash.
That lady Ms. Pipes made a fool out of Bernie Sanders and he deflected in a rage !!
Remember one thing....the current U.S. health insurance system was brought to us by Democrats...100%.
Congressional committee exploratory expeditions about "single" payer systems are meant to bring all facts forward pro and con.
That lady Ms. Pipes made a fool out of Bernie Sanders and he deflected in a rage !!
Remember one thing....the current U.S. health insurance system was brought to us by Democrats...100%.
Congressional committee exploratory expeditions about "single" payer systems are meant to bring all facts forward pro and con.
aboutface
We Canadians love our health care system, despite its annoyances sometimes. What we absolutely hate are the extortionist parking rates in hospital lots.
Although I live in the USA, I also live an hour from the Canadian border on the west coast. The vast majority of Canadians are polite, intelligent, and are reasonably content with their own universal health care system. I never see Canadians utilizing our health care here. Asians and Mexicans and Phillipinos, yes...Canadians no. (parking is a nightmare here, too)
reply to post by Willtell
Canadian 1 - USA 0
I love how Ms. Pipes basically made a fool of herself.
I am proud of that doctor for not letting the American Government spread lies. Damn Im proud to be canadian!
Canadian 1 - USA 0
I love how Ms. Pipes basically made a fool of herself.
I am proud of that doctor for not letting the American Government spread lies. Damn Im proud to be canadian!
reply to post by Willtell
acording to the The Fraser Institute one of canada's leading think tanks. and ranked 22 in the world in 2013. i think the good doctor is blowing smoke.
ranking for The Fraser Institute. page 30 of The Global Go To Think Tank Index PDF. the standard for ranking in the world.
2013 Global Go To Think Tank Index Report
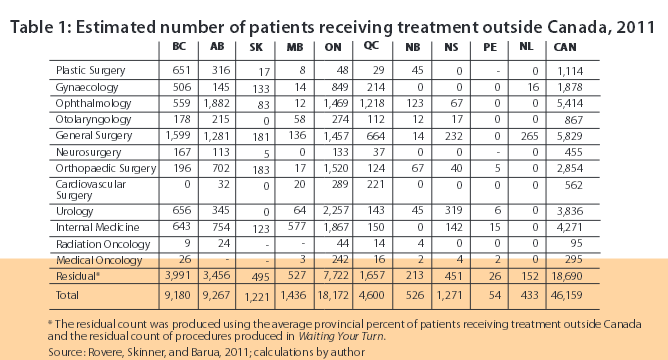
in this 2013Fraser Institute report that shows a estimated 41,838 canadians came to the U.S. for treatment of various kinds.
did you see the key words " conservatively estimated" which means depending on whose definitions you use means,:"cautiously moderate or purposefully low: a conservative estimate".
i read the 2011 report and it stated the number given is likely under estimated and are probably higher due to non reporting/ non referrals,well here is the PDF
i also think that the fact that the economy in canada is as bad everyone elses' is. that maybe the reason for the numbers coming out of canada dropping in 2012 and 2013.
so if we take the years of 2011( see report) 46,159 in 2012 42,173 , and in 2013 41,838 , we get 130,170 canadians came to the U.S. which according to the reports is more than likely under estimated. even you if you just count them as procedures, ie meaning same patient coming for more than one time, that's no small number, and remember that it considered to be a under estimate.
then you have this,
you know 3 months or 9.3 weeks, is a long time to wait to see a doctor.
so clearly the senator asked the wrong questions.
acording to the The Fraser Institute one of canada's leading think tanks. and ranked 22 in the world in 2013. i think the good doctor is blowing smoke.
ranking for The Fraser Institute. page 30 of The Global Go To Think Tank Index PDF. the standard for ranking in the world.
2013 Global Go To Think Tank Index Report
in this 2013Fraser Institute report that shows a estimated 41,838 canadians came to the U.S. for treatment of various kinds.
Putting these numbers together with data on the number of procedures performed in Canada from the Canadian Institute for Health Information reveals that a conservatively estimated 41,838 Canadians received treatment outside the country in 2013.
Interestingly, this year’s estimate is a slight decrease from the 2012 estimate of 42,173. At the same time, the wait time from specialist consultation to treatment in Canada increased from 9.3 weeks in 2012 to 9.6 weeks in 2013.
Seeking relief outside Canada's borders
did you see the key words " conservatively estimated" which means depending on whose definitions you use means,:"cautiously moderate or purposefully low: a conservative estimate".
i read the 2011 report and it stated the number given is likely under estimated and are probably higher due to non reporting/ non referrals,well here is the PDF
The number of patients receiving treatment outside Canada each year produced by this methodology is likely to be an underestimate. This is the result of a few factors. Most importantly, these numbers are based on specialist responses, which means that patients who leave Canada without consulting a specialist are not likely to be included in the count shown in table 1. The counts are also based on the number of procedures estimated to have been performed in Canada, which is less than the total number of patients consulted and less than the total number of Canadians who would have required treatment, including those who left Canada to seek it.
Le aving Canada for medical care 2011
i also think that the fact that the economy in canada is as bad everyone elses' is. that maybe the reason for the numbers coming out of canada dropping in 2012 and 2013.
so if we take the years of 2011( see report) 46,159 in 2012 42,173 , and in 2013 41,838 , we get 130,170 canadians came to the U.S. which according to the reports is more than likely under estimated. even you if you just count them as procedures, ie meaning same patient coming for more than one time, that's no small number, and remember that it considered to be a under estimate.
then you have this,
This edition of Waiting Your Turn indicates that waiting times for elective medical treatment have increased since last year. Specialist physicians surveyed across 12 specialties and 10 Canadian provinces report a total waiting time of 18.2 weeks between referral from a general practitioner and receipt of elective treatment.
Wait times between 2012 and 2013 increased in both the segment between referral by a general practitioner and consultation with a specialist (rising to 8.6 weeks from 8.5 weeks in 2012), and the segment between a consultation with a specialist and receipt of treatment (rising to 9.6 weeks from 9.3 weeks in 2012). While wait times have fallen overall, physicians themselves believe that Canadians wait approximately 3 weeks longer than what they consider is clinically "reasonable" for elective treatment after an appointment with a specialist.
Waiting your turn: Wait times for health care in Canada, 2013 Report
you know 3 months or 9.3 weeks, is a long time to wait to see a doctor.
so clearly the senator asked the wrong questions.
edit on 14-3-2014 by hounddoghowlie because: (no reason given)
edit on 14-3-2014 by hounddoghowlie because: (no reason
given)
reply to post by hounddoghowlie
that is for elective surguries not life threatening surguries. Canadian government does not cover alot of elective surguries because your healthe is not at risk so it is a waste of taxpayer money. Elective surgeries include plastic surgery, tummy tucks, stapped stomaches ect. do not spread false info. For a normal doctors apointment most people have a family doctor that they can make an apointment to see their doctor in just a day or twoo. Also there are emergency rooms and free clinics too. All for the price of $50 a month.
that is for elective surguries not life threatening surguries. Canadian government does not cover alot of elective surguries because your healthe is not at risk so it is a waste of taxpayer money. Elective surgeries include plastic surgery, tummy tucks, stapped stomaches ect. do not spread false info. For a normal doctors apointment most people have a family doctor that they can make an apointment to see their doctor in just a day or twoo. Also there are emergency rooms and free clinics too. All for the price of $50 a month.
reply to post by snypwsd
read the reports and look at the chart.
are all these considered elective surgery. i don't think so maybe in some but not all.
your either going to have your heart fixed or your gonna die.
Ophthalmology,
General Surgery
Neurosurgery
Orthopaedic Surgery
Cardiovascular Surgery
Urology
Internal Medicine
Radiation Oncology
Medical Oncology
and according to the report part of these numbers come from your own government, the Canadian Institute for Health.
read the reports and look at the chart.
are all these considered elective surgery. i don't think so maybe in some but not all.
your either going to have your heart fixed or your gonna die.
Ophthalmology,
General Surgery
Neurosurgery
Orthopaedic Surgery
Cardiovascular Surgery
Urology
Internal Medicine
Radiation Oncology
Medical Oncology
and according to the report part of these numbers come from your own government, the Canadian Institute for Health.
Putting these numbers together with data on the number of procedures performed in Canada from the Canadian Institute for Health Information reveals that a conservatively estimated 41,838 Canadians received treatment outside the country in 2013.
Seeking relief outside Canada's borders
edit on 14-3-2014 by hounddoghowlie because: (no reason given)
reply to post by Willtell
And if he did some more research, specifically dealing with how to pay, they would see that the number of exceptions Obama has handed out has now placed the system into even more chaos. Every time he issues an exemption, it takes money out of the system. That money was "key" in terms of bringing down overall cost for anyone in the system.
Not anymore...
Secondly, when you have Canadians crossing the border into the US to have treatments, it makes one wonder as to why they cant get the same treatment in Canada.
Rationing comes to mind...
And if he did some more research, specifically dealing with how to pay, they would see that the number of exceptions Obama has handed out has now placed the system into even more chaos. Every time he issues an exemption, it takes money out of the system. That money was "key" in terms of bringing down overall cost for anyone in the system.
Not anymore...
Secondly, when you have Canadians crossing the border into the US to have treatments, it makes one wonder as to why they cant get the same treatment in Canada.
Rationing comes to mind...
dup
edit on Friam3b20143America/Chicago18 by Danbones because: (no reason given)
shouldice clinic is a good example
when i went there for a hernia there were private payers from the us at 50%can 50%us
we had our healthcare paid for, the americans paid out of pocket and were happy too
at the time:
Shouldice 97 percent success rate
regular hospitals, canadian included ....the exact opposite
that was early 80s
i have waited a year for cardiac surgery why?
SERVICE CANADA screwed up a replacement birth certificate.
and that burns my butt...i can't complain about my health care because so far
I haven't gotten any
oh well...i have a swiss army knife..it's pretty sharp...boil some water...get some rags...a big bowl ..ats instrutctible...
purpose of obama care..same as the carbon tax
the us has a industrial military complex war effort to pay for and bankers to shine
yes we have clinics and for most stuff they are quick and do the job
emerge departments pretty good
not like they are full of illegals who are first in line
i am being served by Chigamick for integrated care they are good for the basic gp or nurse practitioner type stuff
they integrate into the community support too, out patients housing, Ontario disability support, for those who are out of work because of illness...
we did switch to biometric ids cards because there were hundreds of thousands of counterfit OHIP cards floating around the northern us and those people were coming up here to steal our health care
when i went there for a hernia there were private payers from the us at 50%can 50%us
we had our healthcare paid for, the americans paid out of pocket and were happy too
at the time:
Shouldice 97 percent success rate
regular hospitals, canadian included ....the exact opposite
that was early 80s
i have waited a year for cardiac surgery why?
SERVICE CANADA screwed up a replacement birth certificate.
and that burns my butt...i can't complain about my health care because so far
I haven't gotten any
oh well...i have a swiss army knife..it's pretty sharp...boil some water...get some rags...a big bowl ..ats instrutctible...
edit on Friam3b20143America/Chicago56 by Danbones because: (no reason given)
purpose of obama care..same as the carbon tax
the us has a industrial military complex war effort to pay for and bankers to shine
edit on Friam3b20143America/Chicago22 by Danbones because: (no reason given)
yes we have clinics and for most stuff they are quick and do the job
emerge departments pretty good
not like they are full of illegals who are first in line
i am being served by Chigamick for integrated care they are good for the basic gp or nurse practitioner type stuff
they integrate into the community support too, out patients housing, Ontario disability support, for those who are out of work because of illness...
edit on Friam3b20143America/Chicago45 by Danbones because: (no reason given)
we did switch to biometric ids cards because there were hundreds of thousands of counterfit OHIP cards floating around the northern us and those people were coming up here to steal our health care
edit on Friam3b20143America/Chicago49 by Danbones because: (no reason
given)
edit on Friam3b20143America/Chicago02 by Danbones because: (no reason given)
reply to post by WatchingFromtheShadows
Star for you.
ObamaCare as it stands now is awful. It is isn't worth it in it's current form and has major implications financially. If serious reforms are taken now and it is overhauled early on in a more well thought out manner it could serve The American people more appropriately. There are plenty of Nations that can be studied and used as an example of what works and what does not work.
To me, ObamaCare was pushed through just for the sake of getting it through to start a bigger implementation. What we need to do now is halt all of the waste, and adverse effects and major implications and overhaul it now and model it into something we know can work without harming Use Citizens financially or medically.
Star for you.
ObamaCare as it stands now is awful. It is isn't worth it in it's current form and has major implications financially. If serious reforms are taken now and it is overhauled early on in a more well thought out manner it could serve The American people more appropriately. There are plenty of Nations that can be studied and used as an example of what works and what does not work.
To me, ObamaCare was pushed through just for the sake of getting it through to start a bigger implementation. What we need to do now is halt all of the waste, and adverse effects and major implications and overhaul it now and model it into something we know can work without harming Use Citizens financially or medically.
edit on 3-14-2014 by Flint2011 because: (no reason given)
reply to post by hounddoghowlie
Your source is a conservative right wing think tank.
You can get better information from the typical gossip mag.
Obama care is as bad as republicans could make it.
Your source is a conservative right wing think tank.
You can get better information from the typical gossip mag.
Obama care is as bad as republicans could make it.
That info from the Fraser Institute -- is the Cdn equivalent of the drivel pushing the Obamacare - bought and paid for propaganda.
Apples to apples people: Universal Health Care is an idea that was brought in under controversy but honed and borne just 51 years ago in Canada. At least 3 generations of Canadians have known nothing about the need to pay because you're sick.
Universal Health Care in Canada is being dismantled piece by piece and disseminating into the old US-style of delivering services.
It is being done so in the name of money.
In the video the OP provided, the Cdn doctors are clearly representing the Canadian people... NOT the ones who stand to make fortunes with private care.
Apples to apples people: Universal Health Care is an idea that was brought in under controversy but honed and borne just 51 years ago in Canada. At least 3 generations of Canadians have known nothing about the need to pay because you're sick.
Universal Health Care in Canada is being dismantled piece by piece and disseminating into the old US-style of delivering services.
It is being done so in the name of money.
In the video the OP provided, the Cdn doctors are clearly representing the Canadian people... NOT the ones who stand to make fortunes with private care.
new topics
-
One Flame Throwing Robot Dog for Christmas Please!
Weaponry: 19 minutes ago -
Don't take advantage of people just because it seems easy it will backfire
Rant: 33 minutes ago -
VirginOfGrand says hello
Introductions: 1 hours ago -
Should Biden Replace Harris With AOC On the 2024 Democrat Ticket?
2024 Elections: 1 hours ago -
University student disciplined after saying veganism is wrong and gender fluidity is stupid
Education and Media: 4 hours ago -
Geddy Lee in Conversation with Alex Lifeson - My Effin’ Life
People: 5 hours ago -
God lived as a Devil Dog.
Short Stories: 5 hours ago -
Police clash with St George’s Day protesters at central London rally
Social Issues and Civil Unrest: 7 hours ago -
TLDR post about ATS and why I love it and hope we all stay together somewhere
General Chit Chat: 8 hours ago -
Hate makes for strange bedfellows
US Political Madness: 10 hours ago
top topics
-
Hate makes for strange bedfellows
US Political Madness: 10 hours ago, 18 flags -
Who guards the guards
US Political Madness: 13 hours ago, 13 flags -
Police clash with St George’s Day protesters at central London rally
Social Issues and Civil Unrest: 7 hours ago, 8 flags -
TLDR post about ATS and why I love it and hope we all stay together somewhere
General Chit Chat: 8 hours ago, 7 flags -
University student disciplined after saying veganism is wrong and gender fluidity is stupid
Education and Media: 4 hours ago, 7 flags -
Should Biden Replace Harris With AOC On the 2024 Democrat Ticket?
2024 Elections: 1 hours ago, 4 flags -
Has Tesla manipulated data logs to cover up auto pilot crash?
Automotive Discussion: 14 hours ago, 2 flags -
Don't take advantage of people just because it seems easy it will backfire
Rant: 33 minutes ago, 2 flags -
Geddy Lee in Conversation with Alex Lifeson - My Effin’ Life
People: 5 hours ago, 2 flags -
God lived as a Devil Dog.
Short Stories: 5 hours ago, 2 flags
active topics
-
One Flame Throwing Robot Dog for Christmas Please!
Weaponry • 1 • : Sookiechacha -
Should Biden Replace Harris With AOC On the 2024 Democrat Ticket?
2024 Elections • 23 • : worldstarcountry -
Don't take advantage of people just because it seems easy it will backfire
Rant • 1 • : worldstarcountry -
Thousands Of Young Ukrainian Men Trying To Flee The Country To Avoid Conscription And The War
Other Current Events • 121 • : NorthOS -
University student disciplined after saying veganism is wrong and gender fluidity is stupid
Education and Media • 17 • : DBCowboy -
-@TH3WH17ERABB17- -Q- ---TIME TO SHOW THE WORLD--- -Part- --44--
Dissecting Disinformation • 632 • : daskakik -
So I saw about 30 UFOs in formation last night.
Aliens and UFOs • 43 • : DaydreamerX -
"We're All Hamas" Heard at Columbia University Protests
Social Issues and Civil Unrest • 261 • : YourFaceAgain -
Why did Phizer team with nanobot maker
Medical Issues & Conspiracies • 18 • : annonentity -
Geddy Lee in Conversation with Alex Lifeson - My Effin’ Life
People • 4 • : underpass61