It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

Trump Admits He Takes Hydroxycloroquine
page: 14share:
Look for this medication to become a schedule 1 substance in ~20 or so states
What I'd like to know is whether or not quinine can do function nr.4 of HCQ and CQ explained in the video above, in any reasonably comparable manner given it's increased toxicity over HCQ (in other words, can you still take enough quinine for that effect to be somewhat useful). Of course, HCQ would be preferred, being so much less toxic, invasive, or harmful and therefore being able to be taken in larger quantities, but HCQ is completely blocked from access. Quinine however is freely available in somewhat decent quantities in supplements (200mg if following the recommended daily dose on the label) in my country.
Function nr.4 is the main function for prophylaxis (also referred to as the "third point" at the end of the video).
This video is from April 18, 2020; I wonder if it's also a new product, the quantities of quinine per capsule (recommended usage 3 capsules per day) are much higher than I thought supplements had. I already knew the quantity of quinine in tonic water was severely reduced some years ago and that it became a prescription drug, in the US at least, I figured that was the same in my country. Apparently not (depending on the quantity perhaps, but 200mg is not far of from the 300mg tablets sold by prescription; Plaquenil/HCQ comes in 200mg pills):
Whoever wrote the post below seems to think that quinine does do all the same things as CQ/HCQ (CQ less toxic than quinine, HCQ less toxic than CQ), but if you look at the scientific article referred to as [4], it's actually only associating the mechanism in relation to sialic acid and the ACE-2 receptors with CQ and HCQ, they don't actually spell out that mechanism specifically for quinine, as he describes it below:
I'm not recommending anything, just passing this along from another post that seemed to have some understanding of how quinine (and chloroquine and hydroxychloroquine work).
...
Quinine acts against malaria by targeting its purine nucleoside phosphorylase enzyme (PfPNP) [3], but it has other effects in the body which act against coronavirus.
Namely, it targets angiotensin-converting enzyme 2 (ACE2) [4], interfering with sialic acid biosynthesis [4]. SARS, MERS and Covid-19 use sialic acid moieties as receptors, so quinine (and its synthetic counterparts) prevent viral attachment to cell receptors. [whereislogic: the main function for prophylaxis]
Hydroxychloroquine / Chloroquine / quinine can also act on the immune system through cell signalling and regulation of pro-inflammatory cytokines. [4]
...
[4] New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19? - ScienceDirect
Source: Information on quinine, etc....FWIW | CRMD Message Board Posts
Now if you'll note, that article [4] only talks about the mechanism of action of CQ and HCQ, not quinine. So can anyone help me figure this out? Is the person who said the above (remember it's copy-pasted from elsewhere, so it's actually 2 persons running with it there) right or wrong about quinine? Plus the other questions I already asked that I'm wondering about. Any help woud be appreciated (please spare me the media or Big Pharma talking points and arguments if you feel the urge).
It's a bit ridiculous that the health care system, the bureaucracy, politicians, the government, Big Pharma and the media backing their play, are forcing me to go with the more toxic and less effective version of this substance. Still sounds a lot better than doing nothing and waiting until it's my turn to get my free prize of permanent lung damage, courtesy of the system of things (and people not taking this seriously enough by means of media conditioning, being unnecessarily careless and unwilling to make even the most minor of adjustments to mitigate the risk of spread. By design again).
edit on 29-5-2020 by whereislogic because: (no reason given)
originally posted by: whereislogic
What a surprise, another negative marketing/sales-pitch report. More to follow, as predicted.
All produced by scientists who were quiet about the blatant bias and scientific fraud concerning the VA study, providing evidence that none of their publications can be trusted in the future.
...
And as also predicted before, the newer reports will be much better at giving the appearance of being legit and having no conflict of interest compared to the VA study (which almost looks intentional, the VA study was so blatantly corrupt and deceitful, that any negative report about HCQ thereafter looks like a scientific gem of integrity in comparison, even though it's just more of the same, but dressed better), where almost halve the scientists on that study are known to have received funding from Gilead or otherwise have significant financial ties with Gilead (Remdesivir).
Here's the last time I responded to another one of these attempts to present these marketing/sales-pitch reports under the marketinglabel "Science":
originally posted by: whereislogic
a reply to: Grimpachi
...
The New England Journal of Medicine (your source of publication) has lost all credibility. Anyone who thinks they've got something worth your while to publish, check out the 2nd video of Dr. Raoult for a response to the NEJM and their behaviour in terms of scientific integrity and honesty vs a conflict of interest with Big Pharma pulling the strings.
From the piece you quoted yourself, as if you don't even get how such a negative marketing/sales-pitch report works:
Hydroxychloroquine-treated patients were more severely ill at baseline than those who did not receive hydroxychloroquine...
Basically the same trick as the VA study. ...
originally posted by: whereislogic
a reply to: Phage
Here's my prediction [edit: expectation] regarding the ongoing (mostly) government-funded clinical trials ...:
Each and every one will paint a negative picture on HCQ's already well-established and proven effectiveness both as a prohylaxis and treatment of Covid-19 (more so when optimized with ...).
... How can I know ahead of time that none will send out the message that HCQ has clear benefits (that outweigh any minimal risks concerning QT prolongation, i.e, ventricular arrhythmia*)? Even though frontline experience and honest statistics have already shown clear benefits in spite of all the denial that we already have sufficient data and don't need manipulated so-called "randomized clinical trials" that are really better described as marketing/sales-pitch reports once they are published (again by publishers who said nothing about the VA study akin to what Dr. Raoult had to say about it)? Why is NEJM still in business publishing so-called "scientific articles"? NEJM = The New England Journal of Medicine (who published something about Remdesivir, as discussed by Dr. Raoult in the video of my longer comment on the previous page, and was also the publisher of the article about HCQ that Grimpachi brought up in another thread, another favorite publication of the mainstream media, in particular on the left).
*: something easily fixed in those extremely rare cases where it does occur, by switching from Azithromycin to Doxycycline, showing that it's not HCQ that is the problem here; not to mention all the other drugs that are prescribed for minor issues that also can cause QT prolongation, psych drugs that often do more harm than good for actual unproven benefits. Used all the time with no one complaining about how dangerous they are.
The NEJM is at it again...now they're arguing that HCQ has no prophylactic value. And of course, the media is quick to jump on board. Not a word about the South Korean prophylactic study with 211 cases that I either mentioned in this thread or another (which btw, is so utterly contradictory to the results they are publishing now, that they cannot be reconciled, either the ones who published the statistics for the South Korean study are lying, or the NEJM is, which one of those has actually already proven to be highly unreliable and to eagerly lie, fudge, twist and/or manipulate the statistics by means of protocol* for marketing motives concerning Big Pharma?) *: for example by just giving them a false positive as a testresult for the coronavirus, that'll skewer the numbers in the direction you want them to go, or not giving HCQ at all but just saying that you did, who's going to tell? None of the murderers in hospitals that have denied HCQ to patients or argued against using it as a prophylaxis for themselves so that health care workers like themselves don't have to be the biggest spreaders of this disease, something they couldn't care less about which they demonstrated by arguing against the use of HCQ as a prophylaxis and now participating in publications that are supposed to cover their asses for that selfish behaviour and nagging about QT prolongation).
My expectation seemed to have been correct.
But I'm wondering, is there any reason someone can think of why anyone should trust any sort of statistics or publication by the NEJM on this subject after the crap they've already pulled, or why anyone should trust the type of scientists, hospitals or doctors whose statistics they are claiming to have published?
Or in other words: Why is the NEJM still in business publishing so-called, so-perceived or so-marketed "scientific articles"? Why do people still take them as a serious scientific source and not a marketing company which they've clearly already proven to be?
Dr. Raoult's response to the NEJM (regarding another article that was published but it's just more of the same, slightly better dressed up, plus more importantly, they haven't been honest about what marketing techniques were used in the article responded to below, showing their dishonesty and lack of scientific integrity, or any integrity for that matter):
General tip: never ever trust anything being published by the NEJM or the Lancet ever again. There is no good reason to as long as they're quiet about the article responded to above and their true motivation for publishing it (or staying quiet about it, not mentioning the blatant deceptive marketing and propaganda techniques employed).
edit on 3-6-2020 by whereislogic because: (no reason given)
We used a pragmatic approach to recruitment and follow-up of participants through Internet-based self-referral and online follow-up surveys, and we couriered the trial interventions directly to participants’ homes.
Source: A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19 | NEJM
I'm thinking: If Big Pharma can have chatbots argue against the use of HCQ on the internet (which they have), why wouldn't they be able to make completely fictitious participants to enroll in this study, not take the HCQ and then report that they had Covid-19 symptoms? That's how they counted in that study, most were not tested for Covid-19 at the end of the 14-day trial period. In total they reported only 11 out of 49 in the HCQ group as "Laboratory-confirmed diagnosis" instead of 'suspected based on symptoms' (see Table 2). Of course, how many out of those 11 just said so when filling out a survey on the internet or responding to an e-mail? How many of those can we actually be sure are, one, real and honest people who actually took HCQ and actually received a positive PCR test, and two, actually received real HCQ and not something else delivered as HCQ to the physicians sending it to the participants so that those sending the drugs per mail wouldn't even know any better, and also not those collecting the data, or how many of those 11 actually followed the whole protocol (all 19 tablets)?
Full adherence to the trial intervention differed according to trial group, with 75.4% of participants in the hydroxychloroquine group (312 of 414)...all 19 prescribed tablets...
So 25% didn't follow the whole protocol of 19 tablets. According to these stats that is, which are already unreliable. So could it be all 11? You got almost a 100 candidates there, could be all 11. Of course they won't specify further in the article if that's the case, and since they didn't specify further...
The suspected Covid-19 cases after 14 days based on symptoms is an even shadier number.
These 11 real people that should be involved in that number of "Laboratory-confirmed diagnosis" (assuming that's referring to a positive PCR test, but they're being a little vague about it), I'd like to hear all their testimonies and see their faces. Then I can start thinking about whether or not they were actually given HCQ or whether or not they themselves are honest about taking it, honest about getting a PCR test, or wether or not the result of these PCR tests can be relied upon (whether or not those doing them can be trusted to give honest results). Then I can start thinking about whether or not whatever was detected and identified as the virus being present in a patient, was just some remnant of the virus with which they had already been infected prior to taking HCQ (or what was claimed to be HCQ at least).
That's what you get when publishers like the NEJM are known to publish articles that are intentionally deceptive for marketing purposes, with physicians and hospitals backing their play (Big Pharma's play). Utter and complete skepticism.
Also note that the prophylactic protocol only lasted 5 days and the prophylactic effect of HCQ diminishes since your last dosage. The South Korean protocol was a little different. Nevertheless, the South Korean study also looked at the results after 14 days, they had 205 participants in which the protocol was entirely completed, and 0 "Laboratory-confirmed diagnoses" (PCR positive tests in their case) after 14 days (and I think also 0 suspected cases based on symptoms, but could be that they didn't look at that because it's so unreliable).
So here we have 312 participants who completed the protocol, with 11 "Laboratory-confirmed diagnoses" and 38 more counted as having the disease based on symptoms, a whopping 3.5% and 15,7% (all 49 counted as having the disease after 14 days) respectively, based on the 312 number, so if not counting those who did not complete the protocol, which confusingly are possibly not excluded from the 49 number, i.e. these 49 could include those who did not complete the protocol, in which case the percentages would be different, normally, like in the South Korean study, you would exclude those who didn't complete the HCQ protocol; yet in a study with 205 participants (almost as much) we have 0 positive PCR-tests and possibly 0 suspected cases based on symptoms after 14 days, 0% and 0% respecitively. Why the massive difference? Surely they can't both be right; for neither study the argument can be used that there were simply not enough participants cause they have similar number of participants following the whole protocol. Either one must be manipulating the numbers with unreliable data or not emphasizing inconvenient facts and their related flaws and mistaken impressions they can give.
I think I know which numbers are less reliable based on history and marketing motive. And is anyone ever going to add any zinc? Also note, in the NEJM study, there is only 1 hospitalization in the HCQ group and 0 deaths. So positive or not, they didn't have to be admitted to the hospital, except for that 1 case that may or may not be a real person. I have not seen their testimony, if it's only 1, it should be easy to include along with this study. So we can evaluate whether or not that person comes across as not doing Big Pharma's bidding or being manipulated to do so without realizing. Or whether or not they followed the protocol completely. Whether or not they contracted the disease after a week or so of not taking any HCQ (according to the protocol), which would make sense.
Of course, it won't help us figure out whether or not what he/she was given as HCQ (recorded in the study as HCQ) was actually HCQ.
Another question just came to mind, what if any of these 11 or 49 were given or taking something else as well that makes them more susceptible to the corona virus, or counteracts the mechanism of action of HCQ? Another way to sabotage the results and give a false impression.
Coming back to the very first question in this comment, is there any reason to think that Big Pharma cannot find some actual people to do everything I ascribed to fictituous people there? Seeing it has already proven through the media and politics to be capable of shaping people's opinion about HCQ and make them willing to lie about it and manipulate any clinical trial against the use of HCQ in any form, either as a prophylactic or treatment (by means of the tactics I described in my first question and by means of the motive of covering their own asses for not having used HCQ in the prevention and treatment of Covid-19; lots of health care workers as participants in that study that classify for involuntary manslaughter due to criminal negligence like that, those that have a motive for covering their own asses by giving the impression that HCQ doesn't work anyway, so they supposedly did nothing wrong for withholding it and exaggerating the side effects in comparison to downplaying the benefits, to play along with or to support the argument that benefits are not sufficiently proven or evidenced enough to outweigh the side effects or toxicity)?
What does match between the NEJM and South Korean studies is the following though (which contradicts the claims made in news articles about the Lancet study that was negative about HCQ and associated it with a massive increase in cardiac arrhythmia, compared to Dr. Raoult's observations for example:)
No arrhythmias or deaths occurred. ... Nausea, loose stools, and abdominal discomfort were the most common side effects. There were no serious intervention-related adverse reactions or cardiac arrhythmias.
Source: A Randomized Trial of Hydroxychloroquine as Postexposure Prophylaxis for Covid-19 | NEJM
edit on 4-6-2020 by whereislogic because: (no reason given)
It also shouldn't be that hard for Big Pharma to find 11 people doing a bit of play-acting on camera (or to fool them with a false positive test as
reported by other unreliable lab researchers with dependency on Big Pharma and a conflict of interest as a motive to provide false positives). But I
have a feeling they can't even be bothered to do that to back up their claims about these 11 "Laboratory-confirmed diagnoses". So we'll just have to
take their word for it, which I can't after the earlier marketing articles in the NEJM concerning HCQ and Remdesivir that I referred to earlier (the
Remdesivir one responded to by Dr. Raoult, but not retracted or apologized for by the NEJM, let alone acknowledging their obvious marketing and
advertizing motive and conflict of interest with Big Pharma in favor of the utterly useless and harmful Remdesivir).
edit on 4-6-2020 by
whereislogic because: (no reason given)
Some comments from Twitter about the latest NEJM study about HCQ:
The folic acid one is a big issue, obviously, the placebo has to actually be a placebo, not something that has reported activitity against Sars-Cov-2, then it's not a placebo. Of course, the lack of molecular testing and counting suspected cases was already brought up by me earlier, but avoidable if you simply only count the 11 "Laboratory-confirmed diagnoses", assuming those are positive PCR tests at least. Perhaps that's not even the case, which would make these numbers even more unreliable.
Nope, sounds about right. Except for the "may", which is a definite 'yes, it helps fighting it'. But yeah, this little detail can account for any positive PCR test after 14 days, if those were actually there and not merely reported through the internet as explained earlier. Or not actually false positives or forged positives by those reporting on a test (lab researchers, or those handling or interfering with their data; shouldn't be too hard for a Big Pharma paid hacker to change a negative to a positive after the lab researchers are done, happens all the time with doping but then from positive to negative).
Yes, I noticed that as well, if you look at the Twitter post it says: "to be published @NEJM later today", yet below it are already a bunch of press releases with titles like "Hydroxychloroquine, a drug promoted by Trump, failed to prevent healthy people from getting COVID-19 in trial" and "Hydroxychloroquine does not prevent COVID-19 infection if exposed, study says".
Source: Eric Topol op Twitter: "A randomized, placebo controlled trial of hydroxychloroquine for prevention of #COVID19 shows lack of efficacy ...
Yep, that was my biggest gripe in my previous commentary about it. How can we know these are even real people reporting honestly and accurately? How can we know this electronic data wasn't tampered with by outside influences with a motive to do so (Big Pharma)? Or tampered with by inside sources with a similar motive of wanting to cover their own asses for that matter?
Yep, the South Korean study isn't the only one whose statistical results don't even come close to matching the NEJM study, who is lying? These Indian and South Korean researchers or those involved in the NEJM publication again, for the umpteenth time? The results are supposed to at least somewhat match up if all publications are reflective of the reality of the matter (whether HCQ works or not). We're all talking post-exposure prophylaxis here, why does it work in India and South Korea but not in the US, supposedly (if you have to believe these results)?
Yep, brought that up as well, focusing on 1 of those 2 (the one in the HCQ group, who I like to see on camera to do his/her testimony).
All relevant remarks before blindly going along with the news article titles I earlier referred to. That love to jump the gun on this one, cause they've got their precious so-called "randomized double-blinded controlled trial" to wave up in the air as if showing off their excellent report card to their parents. The type I earlier described as being better 'dressed up' than the VA study, but is just more of the same (less recognizable for what it is because of being better dressed up as a 'scientific gem of integrity' compared to the VA study).
Sad, but true.
Oh, earlier I talked about my biggest gripe with this study, but my biggest gripe is actually that it doesn't match up with the other studies concerning HCQ used as post-exposure-prophylaxis, such as the South Korean one with very similar numbers of participants taking HCQ following the protocol completely (312 vs 205 if comparing the NEJM with the South Korean one, linked on the previous page of this thread under the title "Can Post-Exposure Prophylaxis for COVID-19 Be Considered as an Outbreak Response Strategy in Long-Term Care Hospitals? - PubMed"). So either this NEJM publication is giving a false impression, or the other ones that do attribute efficacy to HCQ in this regards are, such as the South Korean one. They can't both (or all if you include other positive reports about HCQ working as a prophylaxis) be reflecting the truth of the matter, one must give a false impression. I know where my money is on, the one with the clearest motive for giving a false impression and a history of promoting a false impression about HCQ. The one that doesn't emphasize the need for actual positive PCR tests before padding the numbers of "probable" infections, an irrelevant number for accurate reliable statistical analysis, but wonderful for manipulation, bias and marketing purposes.
The other aspect of that gripe is that I already expected such negative publications about HCQ based on motive and for marketing purposes. Making me even more skeptical cause I'm not supposed to know the results ahead of time, unless I'm right about their willingness to fudge the numbers to show what they want them to show, and their ability to do that while still maintaining that appearance of a gold standard clinical trial, honest research and science and scientific integrity.
Kevin McKernan
@Kevin_McKernan
·
8 u
The placebo (Folic Acid) has reported activity against SARS-CoV-2.
The lack of molecular testing means it could be underpowered.
80% of symptomatics in contact with CV test neg on qPCR. The majority of patients may have a diff virus.
...
The Role of Folic Acid in the Management of Respiratory Disease Caused by COVID-19
The folic acid one is a big issue, obviously, the placebo has to actually be a placebo, not something that has reported activitity against Sars-Cov-2, then it's not a placebo. Of course, the lack of molecular testing and counting suspected cases was already brought up by me earlier, but avoidable if you simply only count the 11 "Laboratory-confirmed diagnoses", assuming those are positive PCR tests at least. Perhaps that's not even the case, which would make these numbers even more unreliable.
Novak
@Novak51327248
·
15 u
Als antwoord op
@EricTopol
@BallouxFrancois
en 5 anderen
HCQ will not prevent the body from developing antibodies or from catching the virus. But it may help fighting it. What is the point of this study? am I wrong about something?
Nope, sounds about right. Except for the "may", which is a definite 'yes, it helps fighting it'. But yeah, this little detail can account for any positive PCR test after 14 days, if those were actually there and not merely reported through the internet as explained earlier. Or not actually false positives or forged positives by those reporting on a test (lab researchers, or those handling or interfering with their data; shouldn't be too hard for a Big Pharma paid hacker to change a negative to a positive after the lab researchers are done, happens all the time with doping but then from positive to negative).
Babak Javid
@Babak_Javid_Lab
·
16 u
Als antwoord op
@EricTopol
@lauriemcginley2
en 4 anderen
Gotta love the Press release before the data published trend in Covid-times!!
Hakim Dehbi
@HakDehbi
·
12 u
A concerning trend!
Yes, I noticed that as well, if you look at the Twitter post it says: "to be published @NEJM later today", yet below it are already a bunch of press releases with titles like "Hydroxychloroquine, a drug promoted by Trump, failed to prevent healthy people from getting COVID-19 in trial" and "Hydroxychloroquine does not prevent COVID-19 infection if exposed, study says".
Source: Eric Topol op Twitter: "A randomized, placebo controlled trial of hydroxychloroquine for prevention of #COVID19 shows lack of efficacy ...
QAnon, MD, PhD
@RightDoctor
·
16 u
Als antwoord op
@EricTopol
@lauriemcginley2
en 4 anderen
"The study was conducted in an unusual way: over the internet, without patients being seen by study doctors"
Yep, that was my biggest gripe in my previous commentary about it. How can we know these are even real people reporting honestly and accurately? How can we know this electronic data wasn't tampered with by outside influences with a motive to do so (Big Pharma)? Or tampered with by inside sources with a similar motive of wanting to cover their own asses for that matter?
Jaspreet S Photography
@JaspreetSPhoto
·
14 u
Indian study wasn't done on Internet but health care workers were taking it. they said it reduces viral load compared others who were not taking it.
Yep, the South Korean study isn't the only one whose statistical results don't even come close to matching the NEJM study, who is lying? These Indian and South Korean researchers or those involved in the NEJM publication again, for the umpteenth time? The results are supposed to at least somewhat match up if all publications are reflective of the reality of the matter (whether HCQ works or not). We're all talking post-exposure prophylaxis here, why does it work in India and South Korea but not in the US, supposedly (if you have to believe these results)?
JoshticeMed
@jgtm1234
·
14 u
Just skimming it I don't think it was possible to assess the question with the study design and sample size. Only 2 severe cases/hospitalizations in entire study (1 in each group)
Yep, brought that up as well, focusing on 1 of those 2 (the one in the HCQ group, who I like to see on camera to do his/her testimony).
Hakim Dehbi
@HakDehbi
·
12 u
Als antwoord op
@EricTopol
@BallouxFrancois
en 5 anderen
@EricTopol
absence of evidence isn't evidence of absence. When you say "... shows a lack of efficacy", you're falling into this trap. The CI is from - 2 to 7%. This is large and include potentially very large treatment effect (as well as harm), because of a small sample size.
All relevant remarks before blindly going along with the news article titles I earlier referred to. That love to jump the gun on this one, cause they've got their precious so-called "randomized double-blinded controlled trial" to wave up in the air as if showing off their excellent report card to their parents. The type I earlier described as being better 'dressed up' than the VA study, but is just more of the same (less recognizable for what it is because of being better dressed up as a 'scientific gem of integrity' compared to the VA study).
PSK
@psk1510
·
7 u
Als antwoord op
@EricTopol
@sumanthraman
en 5 anderen
Some scientists and doctors must have spent more time in proving ineffectiveness (by hook or by crook) of hydroxychloroquine- then anything good about it. ...
Sad, but true.
Oh, earlier I talked about my biggest gripe with this study, but my biggest gripe is actually that it doesn't match up with the other studies concerning HCQ used as post-exposure-prophylaxis, such as the South Korean one with very similar numbers of participants taking HCQ following the protocol completely (312 vs 205 if comparing the NEJM with the South Korean one, linked on the previous page of this thread under the title "Can Post-Exposure Prophylaxis for COVID-19 Be Considered as an Outbreak Response Strategy in Long-Term Care Hospitals? - PubMed"). So either this NEJM publication is giving a false impression, or the other ones that do attribute efficacy to HCQ in this regards are, such as the South Korean one. They can't both (or all if you include other positive reports about HCQ working as a prophylaxis) be reflecting the truth of the matter, one must give a false impression. I know where my money is on, the one with the clearest motive for giving a false impression and a history of promoting a false impression about HCQ. The one that doesn't emphasize the need for actual positive PCR tests before padding the numbers of "probable" infections, an irrelevant number for accurate reliable statistical analysis, but wonderful for manipulation, bias and marketing purposes.
The other aspect of that gripe is that I already expected such negative publications about HCQ based on motive and for marketing purposes. Making me even more skeptical cause I'm not supposed to know the results ahead of time, unless I'm right about their willingness to fudge the numbers to show what they want them to show, and their ability to do that while still maintaining that appearance of a gold standard clinical trial, honest research and science and scientific integrity.
edit on 4-6-2020 by whereislogic because: (no reason given)
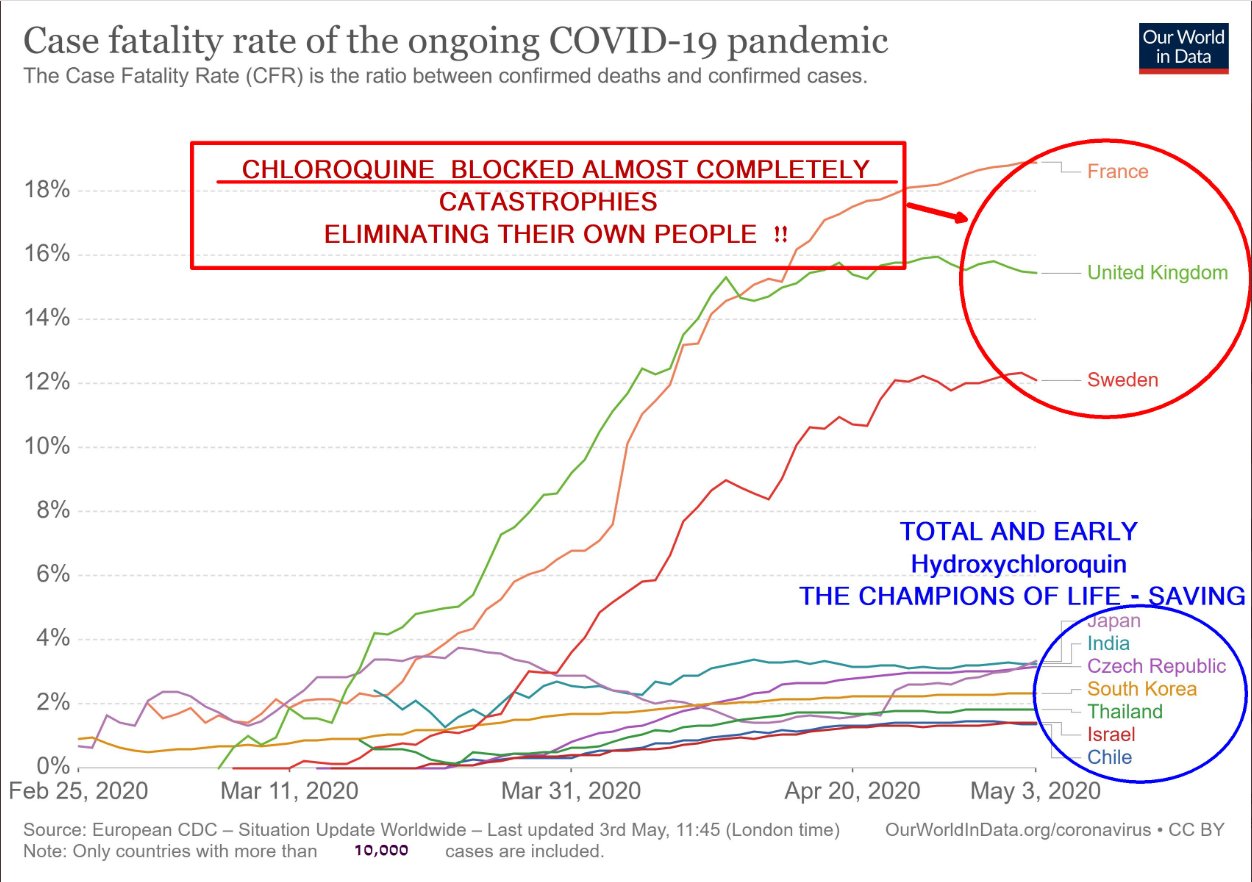
That one was included in one of the responses to that twitter post. Should read hydroxychloroquine in the red box as well of course.
edit on
4-6-2020 by whereislogic because: (no reason given)
It's looking like President Trump was on the right track all along.
twitter.com...
Some people forget that U.S. presidents are privy to information that 99.9% of the population is unaware of. It is up to the president to determine if that information needs to be shared.
Thankfully, President Trump cares about all of us.
twitter.com...
Some people forget that U.S. presidents are privy to information that 99.9% of the population is unaware of. It is up to the president to determine if that information needs to be shared.
Thankfully, President Trump cares about all of us.
a reply to: Sookiechacha
I guess the Doctor was in fact giving him the real goods and it in fact does help for his intended use.
www.abovetopsecret.com...
I guess the Doctor was in fact giving him the real goods and it in fact does help for his intended use.
www.abovetopsecret.com...
edit on 642020 by Butterfinger because: (no reason given)
The Leftist is upset because they know we don't pay attention to a word they say. They're screaming at the sky and the only people listening are their
own kind.
originally posted by: andy06shake
a reply to: JBurns
Can we not just swap Hydroxychloroquine and bring back Methaqualone?
Problem solved, to some degree at least.
Andy, that's a real throwback to the old days :p
It's worth a try
You can only take it for TWO(2) Weeks.
originally posted by: spacedoubt
He stopped taking his drugs.
So he says.
for now he decided to just say no to those drugs.
I think they were messing with his balance, high heels and shoe lifts are a challenge I suppose, under ordinary circumstances.
Just do a bit of research and all your answers will be revealed.
a reply to: spacedoubt
Medication*
Although drugs are technically correct, it carries a negative connotation and is generally reserved for druggies (illegal drug users)
Although I'm sure that was your point
Medication*
Although drugs are technically correct, it carries a negative connotation and is generally reserved for druggies (illegal drug users)
Although I'm sure that was your point
a reply to: Butterfinger
I don't think so. That news does nothing to dispel the reality that Trump's doctor would be breaking FDA rules to prescribe the drug to Trump as an excremental preventative, given the health risks, especially to the heart and knowing Trump's heart disease issues.
I don't think so. That news does nothing to dispel the reality that Trump's doctor would be breaking FDA rules to prescribe the drug to Trump as an excremental preventative, given the health risks, especially to the heart and knowing Trump's heart disease issues.
edit on 5-6-2020 by Sookiechacha because: (no reason given)
WHO resumes trials
The WHO is resuming trials now that its been found not to be the "Devils Tic-tac"
The WHO is resuming trials now that its been found not to be the "Devils Tic-tac"
edit on 652020 by Butterfinger because: (no reason
given)
edit on 652020 by Butterfinger because: (no reason given)
UK trial on hydroxychloroquine: ‘It doesn’t work’
link
Ironically, the WHO who Trump condemns still thinks it might have some use( Though as of now most of the studies say it doesn't work) and will continue to test it.
Yet Trump calls them clueless.
Goes to show us...
Trump is NEVER right about anything
link
A large, randomized U.K. trial found “no clinical benefit” of hydroxychloroquine to treat hospitalized Covid-19 patients, researchers announced Friday.
“It doesn’t work,” declared Martin Landray, one of the lead researchers, at a briefing. Patients receiving hydroxychloroquine died at about the same rate — about one in four — as those receiving regular care in a randomized trial being conducted by the University of Oxford and the U.K. National Health Service.
Ironically, the WHO who Trump condemns still thinks it might have some use( Though as of now most of the studies say it doesn't work) and will continue to test it.
Yet Trump calls them clueless.
Goes to show us...
Trump is NEVER right about anything
edit on 5-6-2020 by Willtell because: (no reason given)
originally posted by: Arnie123
You can only take it for TWO(2) Weeks.
originally posted by: spacedoubt
He stopped taking his drugs.
So he says.
for now he decided to just say no to those drugs.
I think they were messing with his balance, high heels and shoe lifts are a challenge I suppose, under ordinary circumstances.
Just do a bit of research and all your answers will be revealed.
Lupus and Rheuma patients take it for years. It's just that it stays in the body for a while, so as a prophylactic the effects will remain for a while (the efficiency will reduce over time as the HCQ slowly disappears from the body though). His prophylactic protocol probably only lasted for as long as his doctor decided it should last (2 weeks? I don't know). 2 weeks is the time usually used to put someone in quarantaine when they have been exposed, to see if they get the disease. A doctor could decide that the prophylactic use of HCQ should then have a similar time-frame (the time you think the patient might develop the disease).
edit on 5-6-2020 by whereislogic because: (no reason given)
originally posted by: Butterfinger
a reply to: Sookiechacha
Heat disease deaths by HCQ: 0
You forgot to remind people that that 0 number is based on millions of dosages of HCQ prescribed to patients over multiple decades, as also brought out in a study the WHO conducted themselves some time (years?) before the SARS-CoV-2 pandemic. Suddenly they changed their tune.
It makes the 0 number even more impressive when thinking about the safety of taking HCQ (as long as you don't overdose, which counts for pretty much any medicine out there, even supplements or regular types of food, eat too many eggs for too long, and you'll probably get some heart disease deaths as well). Of course, the usual HCQ protocols for Covid-19 (either prophylactic or as a treatment) is peanuts compared to what Lupus and Rheuma take in over multiple years, every day. Mitigating these types of risks (cardiac arrhythmia, qt prolongation and ultimately cardiac deaths in the worst case scenarios) significantly compared to Lupus and Rheuma patients, who are still being prescribed HCQ even after all the negative publications about HCQ supposedly increasing the risks of death caused by qt prolongation followed by cardiac arrhythmia issues and more serious cardiac problems.
The Lancet was quite dishonest in associating HCQ with increased morbidity and mortality due to cardiac arrhythmia issues (actually they said towards the end of the study that one couldn't associate their statisctical study with that, but the news articles went ahead and did that in their titles anyway, and they didn't say anything about that predictable behaviour, given the way they wrote their abstract and the fineprint I just mentioned that can be found much later in the article, which I may have quoted in this thread before). Covid-19 itself causes cardiac arrhythmia issues, with or without HCQ (or HCQ + Azithromycin); so a little dishonest to attribute it to the use of HCQ when looking at Covid-19 patients, as the Lancet study did. This doctor explains:
edit on 5-6-2020 by whereislogic because: (no reason given)
new topics
-
University of Texas Instantly Shuts Down Anti Israel Protests
Education and Media: 1 minutes ago -
Any one suspicious of fever promotions events, major investor Goldman Sachs card only.
The Gray Area: 2 hours ago -
God's Righteousness is Greater than Our Wrath
Religion, Faith, And Theology: 6 hours ago -
Electrical tricks for saving money
Education and Media: 9 hours ago -
VP's Secret Service agent brawls with other agents at Andrews
Mainstream News: 11 hours ago -
Sunak spinning the sickness figures
Other Current Events: 11 hours ago -
Nearly 70% Of Americans Want Talks To End War In Ukraine
Political Issues: 11 hours ago
top topics
-
VP's Secret Service agent brawls with other agents at Andrews
Mainstream News: 11 hours ago, 9 flags -
Cats Used as Live Bait to Train Ferocious Pitbulls in Illegal NYC Dogfighting
Social Issues and Civil Unrest: 15 hours ago, 8 flags -
Electrical tricks for saving money
Education and Media: 9 hours ago, 4 flags -
Nearly 70% Of Americans Want Talks To End War In Ukraine
Political Issues: 11 hours ago, 3 flags -
Sunak spinning the sickness figures
Other Current Events: 11 hours ago, 3 flags -
Late Night with the Devil - a really good unusual modern horror film.
Movies: 13 hours ago, 2 flags -
Any one suspicious of fever promotions events, major investor Goldman Sachs card only.
The Gray Area: 2 hours ago, 2 flags -
The Good News According to Jesus - Episode 1
Religion, Faith, And Theology: 17 hours ago, 1 flags -
God's Righteousness is Greater than Our Wrath
Religion, Faith, And Theology: 6 hours ago, 0 flags -
University of Texas Instantly Shuts Down Anti Israel Protests
Education and Media: 1 minutes ago, 0 flags
active topics
-
University of Texas Instantly Shuts Down Anti Israel Protests
Education and Media • 0 • : FlyersFan -
God's Righteousness is Greater than Our Wrath
Religion, Faith, And Theology • 18 • : andy06shake -
Nearly 70% Of Americans Want Talks To End War In Ukraine
Political Issues • 23 • : andy06shake -
Sunak spinning the sickness figures
Other Current Events • 9 • : Ohanka -
The Acronym Game .. Pt.3
General Chit Chat • 7748 • : bally001 -
HORRIBLE !! Russian Soldier Drinking Own Urine To Survive In Battle
World War Three • 37 • : FlyersFan -
Any one suspicious of fever promotions events, major investor Goldman Sachs card only.
The Gray Area • 3 • : seekshelter -
-@TH3WH17ERABB17- -Q- ---TIME TO SHOW THE WORLD--- -Part- --44--
Dissecting Disinformation • 662 • : F2d5thCavv2 -
SETI chief says US has no evidence for alien technology. 'And we never have'
Aliens and UFOs • 61 • : andy06shake -
The Reality of the Laser
Military Projects • 47 • : F2d5thCavv2