It looks like you're using an Ad Blocker.
Please white-list or disable AboveTopSecret.com in your ad-blocking tool.
Thank you.
Some features of ATS will be disabled while you continue to use an ad-blocker.

The Real Next Level BS of the Vaccine Controversy.
page: 8share:
originally posted by: ElectricUniverse
Should I mention again the fact that several other medical research studies from all over the globe have found the same links that Wakefield and colleagues found?
Dr James Le Fanu
12:01AM GMT 02 Mar 2004
The truth about MMR must be revealed, says Dr James Le Fanu
The Government finds itself in an invidious situation over the MMR/autism controversy, having painted itself into a corner by denying parents the option of the single measles vaccine. They, thus, have no alternative other than to insist the MMR is totally safe - irrespective of evidence that might emerge to suggest the contrary.
Their difficulty is that this position is now looking a lot shakier than it did even a year ago. Several further independent studies have confirmed the association of the syndrome of regressive autism with chronic bowel disorder that was originally described by Andrew Wakefield. More recently, research has confirmed the presence of the measles virus in the gut and spinal fluid of affected children.
This may not constitute "proof" and, indeed, a former colleague of Dr Wakefield challenged the significance of these findings in the Lancet a fortnight ago - and he may be right to do so. None the less, it is beginning to look as if, as neurologist Peter Harvey points out in the same issue, there is now "a step-by-step cascade of evidence" linking the MMR vaccine to some cases of autism.
This could explain the assault on Dr Wakefield's integrity. The validity of his original findings, it is claimed, may have been compromised by a conflict of interest involving research funds that he failed to disclose. This might be relevant if it were true, but it is not, as anyone can check for themselves: Dr Wakefield acknowledged the source of his funding in the Lancet in 1998. It would seem to be that neither the Government nor the medical establishment can afford for Dr Wakefield to be vindicated - and they are getting pretty desperate.
...
www.telegraph.co.uk...
We can even go back to the timeframe that Wakefield and colleagues published their Lancet paper and find similar reports. There were also reports showing this possible link even before the Lancet paper, and before Wakefield et al began to even study this.
In fact, among the many other research papers there is one from Japan in 2000 in which they even found the viral infection from vaccine strains in some of the kids they researched.
Dig Dis Sci. 2000 Apr;45(4):723-9.
Detection and sequencing of measles virus from peripheral mononuclear cells from patients with inflammatory bowel disease and autism.
Kawashima H1, Mori T, Kashiwagi Y, Takekuma K, Hoshika A, Wakefield A.
Author information
Department of Paediatrics, Tokyo Medical University, Japan.
Abstract
It has been reported that measles virus may be present in the intestine of patients with Crohn's disease. Additionally, a new syndrome has been reported in children with autism who exhibited developmental regression and gastrointestinal symptoms (autistic enterocolitis), in some cases soon after MMR vaccine. It is not known whether the virus, if confirmed to be present in these patients, derives from either wild strains or vaccine strains. In order to characterize the strains that may be present, we have carried out the detection of measles genomic RNA in peripheral mononuclear cells (PBMC) in eight patients with Crohn's disease, three patients with ulcerative colitis, and nine children with autistic enterocolitis. As controls, we examined healthy children and patients with SSPE, SLE, HIV-1 (a total of eight cases). RNA was purified from PBMC by Ficoll-paque, followed by reverse transcription using AMV; cDNAs were subjected to nested PCR for detection of specific regions of the hemagglutinin (H) and fusion (F) gene regions. Positive samples were sequenced directly, in nucleotides 8393-8676 (H region) or 5325-5465 (from noncoding F to coding F region). One of eight patients with Crohn disease, one of three patients with ulcerative colitis, and three of nine children with autism, were positive. Controls were all negative. The sequences obtained from the patients with Crohn's disease shared the characteristics with wild-strain virus. The sequences obtained from the patients with ulcerative colitis and children with autism were consistent with being vaccine strains. The results were concordant with the exposure history of the patients. Persistence of measles virus was confirmed in PBMC in some patients with chronic intestinal inflammation.
www.ncbi.nlm.nih.gov...
Let me post that last part again...
...
The sequences obtained from the patients with ulcerative colitis and children with autism were consistent with being vaccine strains. The results were concordant with the exposure history of the patients. Persistence of measles virus was confirmed in PBMC in some patients with chronic intestinal inflammation.
What the UK government was afraid of was that Wakefield's study could show that some of the children from the Lancet 12 were very probably infected with aseptic meningitis that the Urabe strain of the MMR vaccinne was known to have a high risk to cause.
In fact the government of the UK, and their health officials had given indemnization to vaccine manufacturers from any side effects caused from the MMR vaccine, and in specific from the Urabe strain vaccine which was known to be unsafe yet was used from 1988-1992.
(continued below.)
The first link was from 2004 (and is an article, not research) and has now been superseded and can be dismissed due to further research. See below.
The second only shows the presence of the virus and shows no causation.
That would be because the children (not all of them by the way, read the study) had been vaccinated, nothing more.
That study was performed in 2000, this study was performed in 2008.
Lack of association between measles virus vaccine and autism with enteropathy
"What the UK government was afraid of was that Wakefield's study could show that some of the children from the Lancet 12 were very probably infected with aseptic meningitis that the Urabe strain of the MMR vaccinne was known to have a high risk to cause."
Is that your conjecture or have you stolen it from elsewhere?
The urabe strain was replaced in 1992, 6 years before Wakefield's study and the issues with the Urabe strain were already known.
originally posted by: ElectricUniverse
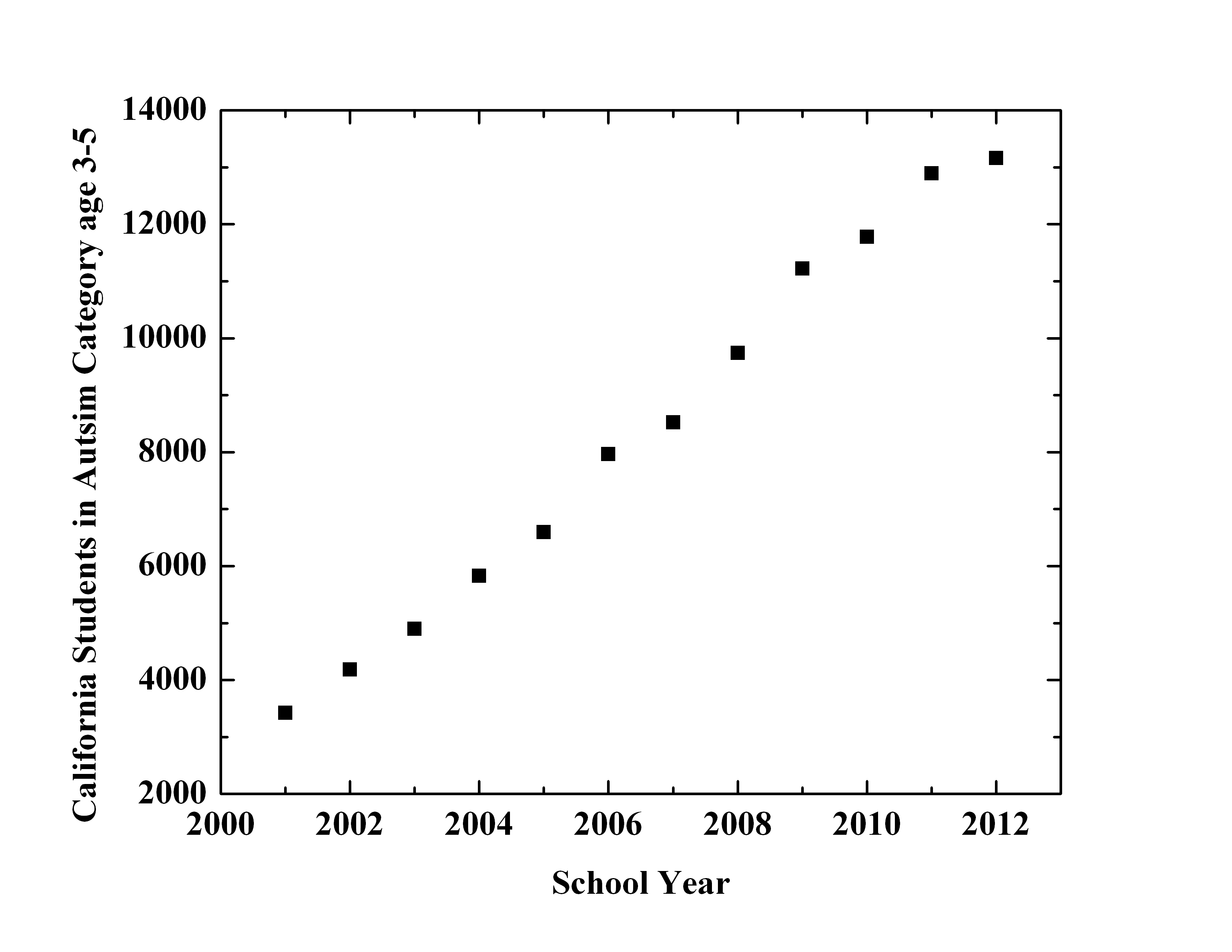
BTW "pardon?" You seem to love to post statistics trying to downplay the rise of children with autism. Now the cases are 1 in 64 for U.S. children to develop autism. Something is causing a trigger. Meanwhile certain vaccines are not the sole trigger, more and more research points to those vaccines you claim are "perfectly safe" could very well be one of the main triggers for the autism epidemic, and other neurological disorders as well as other health problems.
In fact, the figures are really alarming.
If we take for example the rise in cases of autism in children 3-5 years of age in California from 2000-2012
lbrbblog.files.wordpress.com...
Then we have the fact that despite vaccine manufacturers like Merck claiming their vaccines are safer now, we know they have been lying and publishing false information. But of course, like always "pardon?" and a few others will continue to deny all of this...
What I find very interesting is the fact that in the other thread dealing with this subject you try to dismiss several research studies because they say "there is a possibility that vaccines may cause autism, other neurological problems and other health problems. Now you are claiming that Wakefield using similar statements means that he was saying for certain that vaccines do cause these problems?... You like to flip-flop your argument when it fits your agenda...
Correlation does not imply causation.
Diagnosis and reporting are the reasons from the apparent rise in autism.
www.livescience.com...
"Then we have the fact that despite vaccine manufacturers like Merck claiming their vaccines are safer now, we know they have been lying and publishing false information. But of course, like always "pardon?" and a few others will continue to deny all of this..."
If Merck and other vaccine manufacturers lie and provide false information then why do you always point to their vaccine inserts as proof of their harmfulness?
What did you say about "flip-flopping" again?
edit on 4/3/15 by Pardon? because: (no reason given)
a reply to: Pardon?
Let me ask you this. Did the GMC panel, all of them, disclose their conflict of interest in writing?
If you read transcripts from the hearing you would see that some, not all, of the panel chairs disclosed their conflicts of interest, and it wasn't done in writing. It was done by word of mouth right before the hearing.
Wakefield did disclose the possible conflict of interest, and for whatever motive Dr. Horton himself stated he didn't think there was a conflict of interest. After this fiasco things changed on how such conflicts of interest were to be reported.
BTW, how is it that Dr. Horton and the Free Royal Hospital admin weren't aware that Wakefield had been asked to be an expert witness and was to work with Dawbarns solicitors, including Barr, when the £55,000 that Wakefield was to use for research had been dispensed to the Special Trustees of the Hospital Royal Free?
Wakefield did not write the £55,000 check. The Dawbarn solicitors/lawyers/Barr, did. So the Free Royal Hospital admin, and Horton himself must have known that Wakefield was going to be doing research for a legal case. Not to mention the correspondence between Barr and Dr. Horton, in which Barr pointed to Wakefield's past research on this very topic. Dr. Horton must have realized, even if he wasn't told directly by Wakefield which is unlikely, the fact that the lawyers were the ones paying for the research which was to occur after the Lancet paper was ppublished.
www.jabs.org.uk...
It is likely that what Horton claimed about not knowing this was false. This gives credence to Wakefield statements that Horton did indeed know this arrangement.
Let me ask you this. Did the GMC panel, all of them, disclose their conflict of interest in writing?
If you read transcripts from the hearing you would see that some, not all, of the panel chairs disclosed their conflicts of interest, and it wasn't done in writing. It was done by word of mouth right before the hearing.
Wakefield did disclose the possible conflict of interest, and for whatever motive Dr. Horton himself stated he didn't think there was a conflict of interest. After this fiasco things changed on how such conflicts of interest were to be reported.
BTW, how is it that Dr. Horton and the Free Royal Hospital admin weren't aware that Wakefield had been asked to be an expert witness and was to work with Dawbarns solicitors, including Barr, when the £55,000 that Wakefield was to use for research had been dispensed to the Special Trustees of the Hospital Royal Free?
Wakefield did not write the £55,000 check. The Dawbarn solicitors/lawyers/Barr, did. So the Free Royal Hospital admin, and Horton himself must have known that Wakefield was going to be doing research for a legal case. Not to mention the correspondence between Barr and Dr. Horton, in which Barr pointed to Wakefield's past research on this very topic. Dr. Horton must have realized, even if he wasn't told directly by Wakefield which is unlikely, the fact that the lawyers were the ones paying for the research which was to occur after the Lancet paper was ppublished.
Summary of Key Dates and Events
1995 - Dawbarns solicitors of Kings Lynn (employing solicitor Richard Barr) were (along with Freeth Cartwright, another firm of solicitors) appointed by the then Legal Aid Board to manage claims over serious neurological damage (including autism) following MMR.
First quarter of 1997 - Dr Edwards of the Medicines Control Agency wrote privately to Dr Richard Horton, editor of The Lancet, pointing out that Lancet papers’ text and tables were being reproduced by Dawbarns in the “Fact Sheets” provided to parents in the class action.
19th March 1997 - Kirsten Limb at Dawbarns receives a phone call from Sarah Quick at The Lancet, which she marks “urgent” on a memo, referring to Dr Edwards’ written approach to Dr Horton. Dr Edwards is not named at the time, but is named in a subsequent phone call by Sarah Quick at The Lancet.
Sarah Quick tells Kirsten Limb that Dawbarns should apply for retrospective permission to reproduce The Lancet material in Dawbarns’ Fact Sheets to parents. Sarah Quick indicates there should be no problem about granting this permission.
3rd April 1997 - Richard Barr at Dawbarns writes to Dr Horton by fax and by post, explaining Dawbarns’ position. In the coversheet of the fax he makes it clear that his letter to Dr Horton, and correspondence between Barr at Dawbarns and Dr Susan Wood (now deceased) at the Medicines Control Agency were included with the fax, and in addition the Dawbarns Fact Sheet and other original material were being sent to Dr Horton by post.
This letter makes it absolutely clear that Richard Barr works for Dawbarns solicitors and that he is involved in litigation related to potential damage to children following exposure to MMR and measles-rubella vaccines.
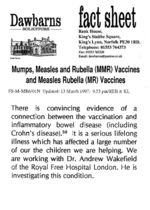
In this letter, Barr also asks Dr Horton for retrospective permission to quote specific Lancet references contained in the Dawbarns Fact Sheet. Barr’s letter specifies the references by number, including reference 50, which is a reference to a paper co-authored by Dr Andrew Wakefield. The text associated with this footnote reads:
‘…There is convincing evidence of a link between vaccination and inflammatory bowel disease including Crohn’s Disease. It is a serious lifelong illness that has affected a large number of the children we are helping. We are working with Dr. Andrew Wakefield of the Royal Free Hospital London. He is investigating this condition…’
Barr thus takes Dr Horton directly to the text that describes Dr Wakefield’s working relationship with Dawbarns and Barr. It is therefore inconceivable that Dr Horton did not scrutinise the precise copyrighted material to which Barr directed Dr Horton.
...
www.jabs.org.uk...
It is likely that what Horton claimed about not knowing this was false. This gives credence to Wakefield statements that Horton did indeed know this arrangement.
edit on 5-3-2015 by ElectricUniverse because: add comment.
originally posted by: Pardon?
Correlation does not imply causation.
That would be correct if only one research paper pointed to the possible harm from certain vaccines.
Coincidences are circumstantial evidence, but if you get enough of them, you have got a case.
The research that Wakefield and colleagues did for the 1998 Lancet study is not the only one pointing to the possibility that certain vaccines can cause adverse health problems such as neurological disorders, inflammation of organs like the brain, and the bowels, etc.
There is a long list of bread crumbs that point to certain vaccines increasing the risk of adverse health problems.
originally posted by: Pardon?
Diagnosis and reporting are the reasons from the apparent rise in autism.
www.livescience.com...
That's one study, from Denmark. I find it quite telling that when it suits you, you point to the conclusions of one study as if that study was proof that the increase in autism cases worldwide must be because diagnosis, and you completely dismiss the plethora of research studies that indicate that certain vaccines may increase the risk of neurological disorders, including regressive autism, alongside other health disorders.
originally posted by: Pardon?
If Merck and other vaccine manufacturers lie and provide false information then why do you always point to their vaccine inserts as proof of their harmfulness?
What did you say about "flip-flopping" again?
I didn't flip-flop. If I point to what vaccine manufacturers "report" is in their vaccines, is to "report what they report". The evidence that certain vaccines can cause harm comes from the plethora of research studies that say so.
edit on 5-3-2015 by ElectricUniverse because: correct comment.
originally posted by: ElectricUniverse
originally posted by: Pardon?
Correlation does not imply causation.
That would be correct if only one research paper pointed to the possible harm from certain vaccines.
Coincidences are circumstantial evidence, but if you get enough of them, you have got a case.
The research that Wakefield and colleagues did for the 1998 Lancet study is not the only one pointing to the possibility that certain vaccines can cause adverse health problems such as neurological disorders, inflammation of organs like the brain, and the bowels, etc.
There is a long list of bread crumbs that point to certain vaccines increasing the risk of adverse health problems.
originally posted by: Pardon?
Diagnosis and reporting are the reasons from the apparent rise in autism.
www.livescience.com...
That's one study, from Denmark. I find it quite telling that when it suits you, you point to the conclusions of one study as if that study was proof that the increase in autism cases worldwide must be because diagnosis, and you completely dismiss the plethora of research studies that indicate that certain vaccines may increase the risk of neurological disorders, including regressive autism, alongside other health disorders.
originally posted by: Pardon?
If Merck and other vaccine manufacturers lie and provide false information then why do you always point to their vaccine inserts as proof of their harmfulness?
What did you say about "flip-flopping" again?
I didn't flip-flop. If I point to what vaccine manufacturers "report" is in their vaccines, is to "report what they report". The evidence that certain vaccines can cause harm comes from the plethora of research studies that say so.
But then there's "possible" harm and proven harm.
Possible is implied from correlation.
Proven is, well, proven.
Your links show NO proof.
It may well be "one study, from Denmark" (although where the study is from is irrelevant) but it clearly shows that the incidence is down to reporting and diagnostic changes.
Tell me why that study is incorrect rather than dismissing it as "one study, from Denmark".
Go on.
"I didn't flip-flop. If I point to what vaccine manufacturers "report" is in their vaccines, is to "report what they report". The evidence that certain vaccines can cause harm comes from the plethora of research studies that say so."
You're right.
You didn't flip=flop.
It's called cherry-picking.
edit on 5/3/15 by Pardon? because: Formatting
originally posted by: ElectricUniverse
a reply to: Pardon?
Let me ask you this. Did the GMC panel, all of them, disclose their conflict of interest in writing?
If you read transcripts from the hearing you would see that some, not all, of the panel chairs disclosed their conflicts of interest, and it wasn't done in writing. It was done by word of mouth right before the hearing.
Wakefield did disclose the possible conflict of interest, and for whatever motive Dr. Horton himself stated he didn't think there was a conflict of interest. After this fiasco things changed on how such conflicts of interest were to be reported.
BTW, how is it that Dr. Horton and the Free Royal Hospital admin weren't aware that Wakefield had been asked to be an expert witness and was to work with Dawbarns solicitors, including Barr, when the £55,000 that Wakefield was to use for research had been dispensed to the Special Trustees of the Hospital Royal Free?
Wakefield did not write the £55,000 check. The Dawbarn solicitors/lawyers/Barr, did. So the Free Royal Hospital admin, and Horton himself must have known that Wakefield was going to be doing research for a legal case. Not to mention the correspondence between Barr and Dr. Horton, in which Barr pointed to Wakefield's past research on this very topic. Dr. Horton must have realized, even if he wasn't told directly by Wakefield which is unlikely, the fact that the lawyers were the ones paying for the research which was to occur after the Lancet paper was ppublished.
Summary of Key Dates and Events
1995 - Dawbarns solicitors of Kings Lynn (employing solicitor Richard Barr) were (along with Freeth Cartwright, another firm of solicitors) appointed by the then Legal Aid Board to manage claims over serious neurological damage (including autism) following MMR.
First quarter of 1997 - Dr Edwards of the Medicines Control Agency wrote privately to Dr Richard Horton, editor of The Lancet, pointing out that Lancet papers’ text and tables were being reproduced by Dawbarns in the “Fact Sheets” provided to parents in the class action.
19th March 1997 - Kirsten Limb at Dawbarns receives a phone call from Sarah Quick at The Lancet, which she marks “urgent” on a memo, referring to Dr Edwards’ written approach to Dr Horton. Dr Edwards is not named at the time, but is named in a subsequent phone call by Sarah Quick at The Lancet.
Sarah Quick tells Kirsten Limb that Dawbarns should apply for retrospective permission to reproduce The Lancet material in Dawbarns’ Fact Sheets to parents. Sarah Quick indicates there should be no problem about granting this permission.
3rd April 1997 - Richard Barr at Dawbarns writes to Dr Horton by fax and by post, explaining Dawbarns’ position. In the coversheet of the fax he makes it clear that his letter to Dr Horton, and correspondence between Barr at Dawbarns and Dr Susan Wood (now deceased) at the Medicines Control Agency were included with the fax, and in addition the Dawbarns Fact Sheet and other original material were being sent to Dr Horton by post.
This letter makes it absolutely clear that Richard Barr works for Dawbarns solicitors and that he is involved in litigation related to potential damage to children following exposure to MMR and measles-rubella vaccines.
In this letter, Barr also asks Dr Horton for retrospective permission to quote specific Lancet references contained in the Dawbarns Fact Sheet. Barr’s letter specifies the references by number, including reference 50, which is a reference to a paper co-authored by Dr Andrew Wakefield. The text associated with this footnote reads:
‘…There is convincing evidence of a link between vaccination and inflammatory bowel disease including Crohn’s Disease. It is a serious lifelong illness that has affected a large number of the children we are helping. We are working with Dr. Andrew Wakefield of the Royal Free Hospital London. He is investigating this condition…’
Barr thus takes Dr Horton directly to the text that describes Dr Wakefield’s working relationship with Dawbarns and Barr. It is therefore inconceivable that Dr Horton did not scrutinise the precise copyrighted material to which Barr directed Dr Horton.
...
www.jabs.org.uk...
It is likely that what Horton claimed about not knowing this was false. This gives credence to Wakefield statements that Horton did indeed know this arrangement.
They're technicalities which weren't the crux of the case and just added to his overall sanctions.
The main points were that Wakefield HIMSELF did not declare any monies paid to him in respect of the legal case on submission of the study.
That is proven.
He did not declare the patent or the link to patient 10's parent's business interest.
That is proven.
He performed unnecessary investigations on disabled children without ethical approval.
That is proven and, in mine and many others' opinions, the most heinous part of it.
Let me ask you this, although Wakefield has been struck off in the UK, he can still practice in other countries given certain stipulations and requirements.
Why then, has he not pursued with his Transfer Factor?
Why hasn't he repeated his study, after all, there's a lot of money in the anti-vaxxers funds for him to be able do it?
Both of those are rhetorical questions.
He hasn't pursued his Transfer Factor as to do so would involve him having to repeat a fraudulent study. One which would no doubt come under intense scrutiny and I doubt he would get away with again.
Add to that there's no recourse and no responsibility for what he does now and his being paid handsomely for being trollied around the US to give his talks and there you have the answer.
The "man's" a fraud who was caught and hasn't got the guts to admit it as to do so would kill his cash-cow.
originally posted by: SlapMonkey
Your last sentence, while true, is not the assumption I made at all. I've repeatedly said that they should take proper precautions--they can still come in to work, but if they know they're succeptible to infections, they would already know how to reduce the possibility of infection, whether you grasp the 'how' behind that or not.
You mean such as asking if the people they regularly come into contact with whether or not they've been vaccinated? A lot of people with compromised immune systems refuse to allow house guests who haven't been - including, obviously, children. That means making the decision to either disclose, or end whatever relationship you have with those people. That's the point I'm getting at - are you happy for that information about you to be potentially made public (at least in the sense of disclosing to other people) in order to help the immuno-compromised among us to make better decisions about their health?
As for ostracizing--I never said they needed to be ostracized, I said they could choose between different options to protect themselves. Don't worry, they'd know how to handle their own life, so I don't need to explain it in detail to you just to satisfy your quest to try and trap me in a revolving discussion that has no end.
I know very well. My boyfriend is on immuno-suppressants due to an organ transplant, and will be for life.
Firstly, I'm only talking about the MMR vaccine, but everything I say about personal choice--whether it be to vaccinate if possible, or to take personal precautions if it's not--is still absolutely valid across the board. The "right to know" if they're potentially at risk is answered in the fact that they cannot undergo the vaccination process. They know they're at risk because they can't be vaccinated. This isn't as difficult a scenario to understand as you are making it out to be, nor is it as big a "load of #" as you're claiming. Also, if you're going to claim that "there are plenty of people out there whose health and wellbeing depends heavily on that of the ones around them," could you provide a link and a number or percentage of the population? I'm willing to bet it's not as high as you're randomly inferring, but if you're going to make such claims, you really should back them up to keep this discussion factual.
I think you misunderstand me a bit here...my point was that whether or not to receive vaccinations isn't always a personal choice, which is what you initially inferred. And unfortunately I can't provide numbers relating to the amount of immunocompromised people out there, because nobody tracks that information. However, considering the number of people with cancer, AIDS, and transplanted organs (and that's not even the full list of everyone who is either immunocompromised or cannot be vaccinated for other reasons), I'd say that number is significant enough to warrant a little consideration from the wider population.
originally posted by: Pardon?
The first link was from 2004 (and is an article, not research) and has now been superseded and can be dismissed due to further research. See below.
I know the difference between an article and a research paper. You keep on trying to derail the topic and I wonder why...
That article that I linked to was written by British physician, medical journalist and author James Le Fanu, in which he explains the same thing I was arguing.
If you need me to point out again what he said, here it is again.
Dr James Le Fanu
12:01AM GMT 02 Mar 2004
...
Their difficulty is that this position is now looking a lot shakier than it did even a year ago. Several further independent studies have confirmed the association of the syndrome of regressive autism with chronic bowel disorder that was originally described by Andrew Wakefield. More recently, research has confirmed the presence of the measles virus in the gut and spinal fluid of affected children.
...
www.telegraph.co.uk...
originally posted by: Pardon?
The second only shows the presence of the virus and shows no causation.
The presence of the virus FROM THE MMR VACCINE... Something which you and some other members claim cannot happen, yet there is the proof that you are once again wrong.
...
. Controls were all negative. The sequences obtained from the patients with Crohn's disease shared the characteristics with wild-strain virus. The sequences obtained from the patients with ulcerative colitis and children with autism were consistent with being vaccine strains. The results were concordant with the exposure history of the patients. Persistence of measles virus was confirmed in PBMC in some patients with chronic intestinal inflammation.
...
originally posted by: Pardon?
That would be because the children (not all of them by the way, read the study) had been vaccinated, nothing more.
That study was performed in 2000, this study was performed in 2008.
Just because a study is done later doesn't negate the findings of older research studies.
But, if you want more recent findings which corroborate my statements, and corroborate other research including those from Japan, here you go.
Eurosurveillance, Volume 18, Issue 49, 05 December 2013
Rapid communications
Case of vaccine-associated measles five weeks post-immunisation, British Columbia, Canada, October 2013
M Murti ()1, M Krajden2, M Petric2, J Hiebert3, F Hemming1, B Hefford4, M Bigham1, P Van Buynder1
Fraser Health Authority, Surrey, British Columbia, Canada
Public Health Microbiology and Reference Laboratory British Columbia Centre for Disease Control, Vancouver, British Columbia, Canada
National Microbiology Laboratory, Public Health Agency of Canada, Winnipeg, Manitoba, Canada
1-1400 George St., White Rock, British Columbia, Canada
Citation style for this article: Murti M, Krajden M, Petric M, Hiebert J, Hemming F, Hefford B, Bigham M, Van Buynder P. Case of vaccine-associated measles five weeks post-immunisation, British Columbia, Canada, October 2013. Euro Surveill. 2013;18(49):pii=20649. Available online: www.eurosurveillance.org...
Date of submission: 15 November 2013
We describe a case of vaccine-associated measles in a two-year-old patient from British Columbia, Canada, in October 2013, who received her first dose of measles-containing vaccine 37 days prior to onset of prodromal symptoms. Identification of this delayed vaccine-associated case occurred in the context of an outbreak investigation of a measles cluster.
In this report we describe a case of measles-mumps-rubella (MMR) vaccine-associated measles illness that was positive by both PCR and IgM, five weeks after administration of the MMR vaccine. Based on our literature review, we believe this is the first such case report which has implications for both public health follow-up of measles cases and vaccine safety surveillance.
...
Laboratory investigations
Laboratory testing for measles was performed on specimens collected on the day of rash onset. Measles RNA was detected in the nasopharyngeal swab by the RT-PCR assay [3]. Acute and convalescent measles specific IgM and IgG antibodies were detected in the blood by ELISA (Enzygnost Anti-Measles Virus IgM and IgG (Dade Behring, Marburg, Germany): IgM detectable (0.213), IgG 1294 mIU/mL, and IgM detectable (0.246), IgG 2,413 mIU/mL, respectively. Virus genotype was determined by the National Microbiology Laboratory in Winnipeg, Canada as vaccine strain, genotype A, MVs/British Columbia/39.13 [A] (VAC) [4]. Other virology testing found no detectable Parvovirus B19 specific IgG or IgM antibody, and detectable human herpesvirus (HHV)-6 specific IgG antibody but no detectable HHV-6 DNA.
www.eurosurveillance.org...
And.
Paediatr Child Health. 2012 Apr; 17(4): e32–e33.
PMCID: PMC3381670
Differentiating the wild from the attenuated during a measles outbreak
Lindsay Nestibo, BN RN,1 Bonita E Lee, MD FRCPC MSC (Epi),2 Kevin Fonseca, PhD D(ABMM),3 Jennifer Beirnes,4 Marcia M Johnson, MD MHSc FRCPC,5 and Christopher A Sikora, MD MSc MPH CCFP FRCPC6
1Communicable Disease Control, Alberta Health Services;
2Paediatric Infectious Disease, University of Alberta;
3Provincial Laboratory for Public Health;
4National Microbiology Laboratory, Public Health Agency of Canada;
5Population and Public Health Division, Alberta Health Services;
6School of Public Health, University of Alberta, Edmonton, Alberta
Correspondence: Dr Christopher A Sikora, University of Alberta, Suite 104 West Tower, Coronation Plaza, 14310–111 Avenue, Edmonton, Alberta T5M 3Z7. Telephone 780-342-0252, e-mail
...
CASE PRESENTATION
In the spring of 2010, there was heightened awareness of measles infection in the physician community as a result of a public health notification related to several imported measles cases in Alberta. During this period, a 15-month-old child presented to his paediatrician’s office with irritability, a fever (38.8°C), a cough and conjunctivitis. The child had a five-day history of illness that began with an elevated temperature and a raised, sandpaper-like rash that originated at the occiput, and eventually spread to and covered the torso. There was mild cervical lymphadenopathy, and no rhinitis or Koplik spots. The child was not immunocompromised and had no significant medical history. Just 12 days before presentation to his paediatrician, the child was immunized with the M-M-R II vaccine (Merck Canada Inc). A thorough investigation by the Division of Population and Public Health, Alberta Health Services, revealed no significant travel history and no contact with any known measles patients in the preceding four weeks. All other members of the household were healthy and previously immunized with an MMR vaccine.
...
Two weeks after the resolution of symptoms, the National Microbiology Laboratory reported the measles virus in both samples as being genotype A – 100% identical to Genbank entry #FJ2111583 (the Edmonston-Enders vaccine strain).
...
www.ncbi.nlm.nih.gov...
edit on 5-3-2015 by ElectricUniverse because: correct post.
To add to this thread, I would like to ask the question: Why would you trust these companies with your health or even worse, your children's
health?
Knowing the lengths these companies will go to make a buck (link below), do they really have your health and safety in mind, especially with immunity granted to them when it comes to vaccine injuries?
projects.propublica.org...
Knowing the lengths these companies will go to make a buck (link below), do they really have your health and safety in mind, especially with immunity granted to them when it comes to vaccine injuries?
projects.propublica.org...
originally posted by: Pardon?
Is that your conjecture or have you stolen it from elsewhere?
It is neither conjecture, nor did i steal it from elsewhere... Again with the ad hominem attacks?
Now Legal Immunity for Swine flu Vaccine Makers
By F. William Engdahl
Global Research, July 20, 2009
30 November -0001
...
According to one independent UK investigator, Alan Golding, who obtained Freedom of Information documents on the case, in “1986 Trivirix, an MMR compound containing the Mumps Urabe strain AM-9, was introduced in Canada to replace MMR I. Concerns regarding the introduction of MMR in the UK are recorded in the minutes of the Joint Working Party of the British Paediatric Association and the Joint Committee on Vaccination and Immunization (JCVI) Liaison Group on June 26th of that year. Such concerns were soon to prove well grounded, as reports began to come in of an increased incidence of aseptic meningitis in vaccinated individuals. Ultimately, all MMR vaccines containing the Urabe strain of mumps were withdrawn in Canada in early 1988. This was before Urabe containing vaccines were licenced by the Department of Health for use in the UK…”
The report adds, “Smith-Kline—French, the pharmaceutical company who became Smith-Kline-Beecham and were involved in UK manufacture at that time, were concerned about these safety issues and were reluctant to obtain a UK license for their Urabe-containing vaccines. As a result of their ‘concern’ that children might be seriously damaged by one of their products, they requested that the UK government indemnify them against possible legal action that might be taken as a result of ‘losses’ associated with the vaccine, which by then was known to carry significant risk to health. The UK government, advised by Professor Salisbury and representatives from the Department of Health, in it’s enthusiasm to get a cheap MMR onto the market, agreed to this request.”
...
www.globalresearch.ca...
originally posted by: Pardon?
The urabe strain was replaced in 1992, 6 years before Wakefield's study and the issues with the Urabe strain were already known.
If you were to read the retracted version of the Lancet study, you would find corroboration of my argument. (I had to download a pdf version of the original Lancet study to read it.)
Here is a version of the retracted Lancet study.
www.thelancet.com...
First of all, the children's age ranged from 3-10 years old at the time of the study at the end of 1997. Median age was 6 years. So, some of the children were old enough to have received the Urabe strain MMR vaccine that health officials in the UK lincensed to be used in the UK even though cases from Canada already showed that this particular strain had a high risk of AM (Aseptic Meningitis), as I proved above. The Urabe strain of the MMR vaccine was withdrawn in 1988, the same year it was approved in the UK. Some of the children from the Lancet study were old enough to have received the Urabe strain MMR vaccine in the UK which was licensed to be used from 1988-1992.
Because of this, children from the Lancet study would have proved that the UK government could be sued because they knew that the cheaper version of the MMR vaccine from the Urabe strain had a high risk of infection of AM(Aseptic Meningitis), and since the UK government indemnified vaccine manufacturers against lawsuits brought by possible damages from the MMR Urabe strain vaccine. This put the government of the UK in the crosshairs, and they couldn't have that, so they made Wakefield the scapegoat.
This is why the UK government officials, vaccine manufacturers and their thugs went against Wakefield so relentlessly.
edit on 6-3-2015 by ElectricUniverse because: correct comment and add link.
originally posted by: Pardon?
But then there's "possible" harm and proven harm.
Possible is implied from correlation.
Proven is, well, proven.
Your links show NO proof.
I see, so when study after study, not linked to MMR vaccine manufacturers as paying the bill, show that vaccines can cause damage "it is not proof"?
Have you forgotten that tobacco MAY cause cancer on people? Heck, there are a lot of smokers who don't get cancer. But I guess for you that's evidence that tobacco CAN'T cause cancer?
The meaning of the words "may", and "possible" don't mean "it doesn't happen".
originally posted by: Pardon?
It may well be "one study, from Denmark" (although where the study is from is irrelevant) but it clearly shows that the incidence is down to reporting and diagnostic changes.
Tell me why that study is incorrect rather than dismissing it as "one study, from Denmark".
Go on.
UC Davis M.I.N.D. Institute study shows California's autism increase not due to better counting, diagnosis
A study by researchers at the UC Davis M.I.N.D. Institute has found that the seven- to eight-fold increase in the number children born in California with autism since 1990 cannot be explained by either changes in how the condition is diagnosed or counted — and the trend shows no sign of abating.
Published in the January 2009 issue of the journal Epidemiology, results from the study also suggest that research should shift from genetics to the host of chemicals and infectious microbes in the environment that are likely at the root of changes in the neurodevelopment of California’s children.
“It’s time to start looking for the environmental culprits responsible for the remarkable increase in the rate of autism in California,” said UC Davis M.I.N.D. Institute researcher Irva Hertz-Picciotto, a professor of environmental and occupational health and epidemiology and an internationally respected autism researcher.
...
www.ucdmc.ucdavis.edu...
edit on 6-3-2015 by ElectricUniverse because: correct post.
Outbreak of Measles Among Persons With Prior Evidence of Immunity, New York City, 2011
Jennifer B. Rosen1,
Jennifer S. Rota2,
Carole J. Hickman2,
Sun Sowers2,
Sara Mercader2,
Paul A. Rota2,
William J. Bellini2,
Ada J. Huang3,
Margaret K. Doll1,
Jane R. Zucker1,2, and
Christopher M. Zimmerman1
- Author Affiliations
1Bureau of Immunization, New York City Department of Health and Mental Hygiene, New York City, New York, U.S.A.
2National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC), Atlanta, GA, U.S.A.
3Westchester County Department of Health, New Rochelle , New York, U.S.A.
Corresponding author: Jennifer Rosen, MD, Address: 42-09 28th St, 5th Fl, CN 21, Queens, NY 11101; Phone: 347-396-2473, Fax: 347-396-2558; Email: [email protected]
Alternate corresponding author: Christopher Zimmerman, MD, MPH, Address: 409 Vanderbilt St, Brooklyn, NY 11218; Phone: 770-371-2093; Email: [email protected]
Abstract
Background. Measles was eliminated in the United States through high vaccination coverage and a public health system able to rapidly respond to measles. Measles may occur among vaccinated individuals, but secondary transmission from such individuals has not been documented.
Methods. Suspected cases and contacts exposed during a measles outbreak in New York City in 2011 were investigated. Medical histories and immunization records were obtained. Cases were confirmed by detection of measles-specific IgM and/or RNA. Tests for measles IgG, IgG avidity, measurement of measles neutralizing antibody titers, and genotyping were performed to characterize the cases.
Results. The index case had two doses of measles-containing vaccine. Of 88 contacts, four secondary cases were confirmed that had either two doses of measles-containing vaccine or a past positive measles IgG antibody. All cases had laboratory confirmation of measles infection, clinical symptoms consistent with measles, and high avidity IgG antibody characteristic of a secondary immune response.
..
Conclusions. This is the first report of measles transmission from a twice vaccinated individual. The clinical presentation and laboratory data of the index were typical of measles in a naïve individual. Secondary cases had robust anamnestic antibody responses. No tertiary cases occurred despite numerous contacts. This outbreak underscores the need for thorough epidemiologic and laboratory investigation of suspected measles cases regardless of vaccination status.
Received November 6, 2013.
Accepted February 9, 2014.
cid.oxfordjournals.org...
There are quite a few cases of "this is the first case that vaccines can cause diseases" isn't?
edit on 6-3-2015 by ElectricUniverse because: (no reason given)
originally posted by: ElectricUniverse
originally posted by: Pardon?
The first link was from 2004 (and is an article, not research) and has now been superseded and can be dismissed due to further research. See below.
I know the difference between an article and a research paper. You keep on trying to derail the topic and I wonder why...
That article that I linked to was written by British physician, medical journalist and author James Le Fanu, in which he explains the same thing I was arguing.
If you need me to point out again what he said, here it is again.
Dr James Le Fanu
12:01AM GMT 02 Mar 2004
...
Their difficulty is that this position is now looking a lot shakier than it did even a year ago. Several further independent studies have confirmed the association of the syndrome of regressive autism with chronic bowel disorder that was originally described by Andrew Wakefield. More recently, research has confirmed the presence of the measles virus in the gut and spinal fluid of affected children.
...
www.telegraph.co.uk...
originally posted by: Pardon?
The second only shows the presence of the virus and shows no causation.
The presence of the virus FROM THE MMR VACCINE... Something which you and some other members claim cannot happen, yet there is the proof that you are once again wrong.
...
. Controls were all negative. The sequences obtained from the patients with Crohn's disease shared the characteristics with wild-strain virus. The sequences obtained from the patients with ulcerative colitis and children with autism were consistent with being vaccine strains. The results were concordant with the exposure history of the patients. Persistence of measles virus was confirmed in PBMC in some patients with chronic intestinal inflammation.
...
originally posted by: Pardon?
That would be because the children (not all of them by the way, read the study) had been vaccinated, nothing more.
That study was performed in 2000, this study was performed in 2008.
Just because a study is done later doesn't negate the findings of older research studies.
Dear me.
The study you originally cited showed that there was MMR virus present.
It did not say it was the cause of anything did it?
The subsequent study showed no causation.
That's why it supersedes it, not because it was done later.
Even though you've quoted the article twice, you've posted nothing backing it up and the writer, a quite prolific writer, has never backed nor followed the piece up.
I keep on seeing this "several further independent studies have confirmed the association of the syndrome of regressive autism with chronic bowel disorder that was originally described by Andrew Wakefield." trop but I never see the studies.
Why is this?
Is it because they don't exist or that they don't actually say what you think they do?
Possibly both.
originally posted by: ElectricUniverse
But, if you want more recent findings which corroborate my statements, and corroborate other research including those from Japan, here you go.
Eurosurveillance, Volume 18, Issue 49, 05 December 2013
Rapid communications
Case of vaccine-associated measles five weeks post-immunisation, British Columbia, Canada, October 2013
M Murti ()1, M Krajden2, M Petric2, J Hiebert3, F Hemming1, B Hefford4, M Bigham1, P Van Buynder1
Fraser Health Authority, Surrey, British Columbia, Canada
Public Health Microbiology and Reference Laboratory British Columbia Centre for Disease Control, Vancouver, British Columbia, Canada
National Microbiology Laboratory, Public Health Agency of Canada, Winnipeg, Manitoba, Canada
1-1400 George St., White Rock, British Columbia, Canada
Citation style for this article: Murti M, Krajden M, Petric M, Hiebert J, Hemming F, Hefford B, Bigham M, Van Buynder P. Case of vaccine-associated measles five weeks post-immunisation, British Columbia, Canada, October 2013. Euro Surveill. 2013;18(49):pii=20649. Available online: www.eurosurveillance.org...
Date of submission: 15 November 2013
We describe a case of vaccine-associated measles in a two-year-old patient from British Columbia, Canada, in October 2013, who received her first dose of measles-containing vaccine 37 days prior to onset of prodromal symptoms. Identification of this delayed vaccine-associated case occurred in the context of an outbreak investigation of a measles cluster.
In this report we describe a case of measles-mumps-rubella (MMR) vaccine-associated measles illness that was positive by both PCR and IgM, five weeks after administration of the MMR vaccine. Based on our literature review, we believe this is the first such case report which has implications for both public health follow-up of measles cases and vaccine safety surveillance.
...
Laboratory investigations
Laboratory testing for measles was performed on specimens collected on the day of rash onset. Measles RNA was detected in the nasopharyngeal swab by the RT-PCR assay [3]. Acute and convalescent measles specific IgM and IgG antibodies were detected in the blood by ELISA (Enzygnost Anti-Measles Virus IgM and IgG (Dade Behring, Marburg, Germany): IgM detectable (0.213), IgG 1294 mIU/mL, and IgM detectable (0.246), IgG 2,413 mIU/mL, respectively. Virus genotype was determined by the National Microbiology Laboratory in Winnipeg, Canada as vaccine strain, genotype A, MVs/British Columbia/39.13 [A] (VAC) [4]. Other virology testing found no detectable Parvovirus B19 specific IgG or IgM antibody, and detectable human herpesvirus (HHV)-6 specific IgG antibody but no detectable HHV-6 DNA.
www.eurosurveillance.org...
And.
Paediatr Child Health. 2012 Apr; 17(4): e32–e33.
PMCID: PMC3381670
Differentiating the wild from the attenuated during a measles outbreak
Lindsay Nestibo, BN RN,1 Bonita E Lee, MD FRCPC MSC (Epi),2 Kevin Fonseca, PhD D(ABMM),3 Jennifer Beirnes,4 Marcia M Johnson, MD MHSc FRCPC,5 and Christopher A Sikora, MD MSc MPH CCFP FRCPC6
1Communicable Disease Control, Alberta Health Services;
2Paediatric Infectious Disease, University of Alberta;
3Provincial Laboratory for Public Health;
4National Microbiology Laboratory, Public Health Agency of Canada;
5Population and Public Health Division, Alberta Health Services;
6School of Public Health, University of Alberta, Edmonton, Alberta
Correspondence: Dr Christopher A Sikora, University of Alberta, Suite 104 West Tower, Coronation Plaza, 14310–111 Avenue, Edmonton, Alberta T5M 3Z7. Telephone 780-342-0252, e-mail
...
CASE PRESENTATION
In the spring of 2010, there was heightened awareness of measles infection in the physician community as a result of a public health notification related to several imported measles cases in Alberta. During this period, a 15-month-old child presented to his paediatrician’s office with irritability, a fever (38.8°C), a cough and conjunctivitis. The child had a five-day history of illness that began with an elevated temperature and a raised, sandpaper-like rash that originated at the occiput, and eventually spread to and covered the torso. There was mild cervical lymphadenopathy, and no rhinitis or Koplik spots. The child was not immunocompromised and had no significant medical history. Just 12 days before presentation to his paediatrician, the child was immunized with the M-M-R II vaccine (Merck Canada Inc). A thorough investigation by the Division of Population and Public Health, Alberta Health Services, revealed no significant travel history and no contact with any known measles patients in the preceding four weeks. All other members of the household were healthy and previously immunized with an MMR vaccine.
...
Two weeks after the resolution of symptoms, the National Microbiology Laboratory reported the measles virus in both samples as being genotype A – 100% identical to Genbank entry #FJ2111583 (the Edmonston-Enders vaccine strain).
...
www.ncbi.nlm.nih.gov...
Here's a quote from the first one.
"It is possible that the case’s symptoms were not measles-vaccine-related but an inter-current illness confounding the presentation. However, symptoms of marked conjunctivitis, continued fever with rash, and progression of macular rash from face to the whole body, are all more suggestive of measles versus other exanthems caused by viral diseases. Parvovirus and HHV-6 results were negative, and the absence of intake of medications excludes a drug reaction. Rubella serology was not done as it was expected to be positive given the recent MMR vaccine administration. Therefore, the combination of classic measles symptoms, detection of measles vaccine virus and reactive measles IgM, and lack of evidence of an alternative illness explanation, were highly suggestive of measles vaccine-associated illness."
One case.
That's ONE single case and the authors are cautious enough to realise that it might not have been measles.
If there were hundreds even tens of cases like this then it would be worth taking note of.
A single case isn't.
For your second link you forgot to include this
"The MMR vaccine contains live attenuated measles virus. It is estimated that administration of this vaccine is associated with moderate (39.4°C) fever in as many as 5% of recipients, and a rash in approximately 2% of those receiving immunization (3). These events typically occur approximately five to 12 days following immunization and often resolve without medical intervention."
So the patient had a common immune response to the ATTENUATED virus.
"An attenuated vaccine is a vaccine created by reducing the virulence of a pathogen, but still keeping it viable (or "live"). Attenuation takes an infectious agent and alters it so that it becomes harmless or less virulent.
So he had the attenuated virus in his urine.
The attenuated virus can't cause measles, it will only be an issue to the recipient and the issue, as has been shown by your link, will be mild and not the measles.
Nothing to do with autism or bowel disorders though...
edit on 6/3/15 by Pardon? because: (no reason given)
originally posted by: ElectricUniverse
originally posted by: Pardon?
But then there's "possible" harm and proven harm.
Possible is implied from correlation.
Proven is, well, proven.
Your links show NO proof.
I see, so when study after study, not linked to MMR vaccine manufacturers as paying the bill, show that vaccines can cause damage "it is not proof"?
Have you forgotten that tobacco MAY cause cancer on people? Heck, there are a lot of smokers who don't get cancer. But I guess for you that's evidence that tobacco CAN'T cause cancer?
The meaning of the words "may", and "possible" don't mean "it doesn't happen".
originally posted by: Pardon?
It may well be "one study, from Denmark" (although where the study is from is irrelevant) but it clearly shows that the incidence is down to reporting and diagnostic changes.
Tell me why that study is incorrect rather than dismissing it as "one study, from Denmark".
Go on.
UC Davis M.I.N.D. Institute study shows California's autism increase not due to better counting, diagnosis
A study by researchers at the UC Davis M.I.N.D. Institute has found that the seven- to eight-fold increase in the number children born in California with autism since 1990 cannot be explained by either changes in how the condition is diagnosed or counted — and the trend shows no sign of abating.
Published in the January 2009 issue of the journal Epidemiology, results from the study also suggest that research should shift from genetics to the host of chemicals and infectious microbes in the environment that are likely at the root of changes in the neurodevelopment of California’s children.
“It’s time to start looking for the environmental culprits responsible for the remarkable increase in the rate of autism in California,” said UC Davis M.I.N.D. Institute researcher Irva Hertz-Picciotto, a professor of environmental and occupational health and epidemiology and an internationally respected autism researcher.
...
www.ucdmc.ucdavis.edu...
Nope.
The difference is that smoking tobacco has been proven to cause cancer.
Whereas there has been no proof ever, that MMR vaccines cause autism.
None.
At all.
If you look at the study I posted from |Denmark, which was published only last year, you can see that the methodology and inclusion criteria were much more robust than the M.I.N.D. one.
It also included (and excluded) more variables making it more pertinent.
The study you posted actually found that at least quarter of all diagnoses were due to diagnostic changes.
Now whether autism is genetic and/or exacerbated by environmental factors is debatable.
One thing that isn't though is that vaccines cause it.
That's been shown to be false.
Lots of times.
originally posted by: ElectricUniverse
Outbreak of Measles Among Persons With Prior Evidence of Immunity, New York City, 2011
Jennifer B. Rosen1,
Jennifer S. Rota2,
Carole J. Hickman2,
Sun Sowers2,
Sara Mercader2,
Paul A. Rota2,
William J. Bellini2,
Ada J. Huang3,
Margaret K. Doll1,
Jane R. Zucker1,2, and
Christopher M. Zimmerman1
- Author Affiliations
1Bureau of Immunization, New York City Department of Health and Mental Hygiene, New York City, New York, U.S.A.
2National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC), Atlanta, GA, U.S.A.
3Westchester County Department of Health, New Rochelle , New York, U.S.A.
Corresponding author: Jennifer Rosen, MD, Address: 42-09 28th St, 5th Fl, CN 21, Queens, NY 11101; Phone: 347-396-2473, Fax: 347-396-2558; Email: [email protected]
Alternate corresponding author: Christopher Zimmerman, MD, MPH, Address: 409 Vanderbilt St, Brooklyn, NY 11218; Phone: 770-371-2093; Email: [email protected]
Abstract
Background. Measles was eliminated in the United States through high vaccination coverage and a public health system able to rapidly respond to measles. Measles may occur among vaccinated individuals, but secondary transmission from such individuals has not been documented.
Methods. Suspected cases and contacts exposed during a measles outbreak in New York City in 2011 were investigated. Medical histories and immunization records were obtained. Cases were confirmed by detection of measles-specific IgM and/or RNA. Tests for measles IgG, IgG avidity, measurement of measles neutralizing antibody titers, and genotyping were performed to characterize the cases.
Results. The index case had two doses of measles-containing vaccine. Of 88 contacts, four secondary cases were confirmed that had either two doses of measles-containing vaccine or a past positive measles IgG antibody. All cases had laboratory confirmation of measles infection, clinical symptoms consistent with measles, and high avidity IgG antibody characteristic of a secondary immune response.
..
Conclusions. This is the first report of measles transmission from a twice vaccinated individual. The clinical presentation and laboratory data of the index were typical of measles in a naïve individual. Secondary cases had robust anamnestic antibody responses. No tertiary cases occurred despite numerous contacts. This outbreak underscores the need for thorough epidemiologic and laboratory investigation of suspected measles cases regardless of vaccination status.
Received November 6, 2013.
Accepted February 9, 2014.
cid.oxfordjournals.org...
There are quite a few cases of "this is the first case that vaccines can cause diseases" isn't?
But if you read the study properly you will see that vaccines HAVEN'T caused the disease.
What the study shows is that a person who had been vaccinated and on whom the vaccination did not work was shown to have contracted and transmitted measles.
"This is the first report of measles transmission from a twice vaccinated individual. The clinical presentation and laboratory data of the index were typical of measles in a naïve individual."
It means that, as we already know, vaccines aren't 100% effective.
originally posted by: ElectricUniverse
originally posted by: Pardon?
Is that your conjecture or have you stolen it from elsewhere?
It is neither conjecture, nor did i steal it from elsewhere... Again with the ad hominem attacks?
Now Legal Immunity for Swine flu Vaccine Makers
By F. William Engdahl
Global Research, July 20, 2009
30 November -0001
...
According to one independent UK investigator, Alan Golding, who obtained Freedom of Information documents on the case, in “1986 Trivirix, an MMR compound containing the Mumps Urabe strain AM-9, was introduced in Canada to replace MMR I. Concerns regarding the introduction of MMR in the UK are recorded in the minutes of the Joint Working Party of the British Paediatric Association and the Joint Committee on Vaccination and Immunization (JCVI) Liaison Group on June 26th of that year. Such concerns were soon to prove well grounded, as reports began to come in of an increased incidence of aseptic meningitis in vaccinated individuals. Ultimately, all MMR vaccines containing the Urabe strain of mumps were withdrawn in Canada in early 1988. This was before Urabe containing vaccines were licenced by the Department of Health for use in the UK…”
The report adds, “Smith-Kline—French, the pharmaceutical company who became Smith-Kline-Beecham and were involved in UK manufacture at that time, were concerned about these safety issues and were reluctant to obtain a UK license for their Urabe-containing vaccines. As a result of their ‘concern’ that children might be seriously damaged by one of their products, they requested that the UK government indemnify them against possible legal action that might be taken as a result of ‘losses’ associated with the vaccine, which by then was known to carry significant risk to health. The UK government, advised by Professor Salisbury and representatives from the Department of Health, in it’s enthusiasm to get a cheap MMR onto the market, agreed to this request.”
...
www.globalresearch.ca...
originally posted by: Pardon?
The urabe strain was replaced in 1992, 6 years before Wakefield's study and the issues with the Urabe strain were already known.
If you were to read the retracted version of the Lancet study, you would find corroboration of my argument. (I had to download a pdf version of the original Lancet study to read it.)
Here is a version of the retracted Lancet study.
www.thelancet.com...
First of all, the children's age ranged from 3-10 years old at the time of the study at the end of 1997. Median age was 6 years. So, some of the children were old enough to have received the Urabe strain MMR vaccine that health officials in the UK lincensed to be used in the UK even though cases from Canada already showed that this particular strain had a high risk of AM (Aseptic Meningitis), as I proved above. The Urabe strain of the MMR vaccine was withdrawn in 1988, the same year it was approved in the UK. Some of the children from the Lancet study were old enough to have received the Urabe strain MMR vaccine in the UK which was licensed to be used from 1988-1992.
Because of this, children from the Lancet study would have proved that the UK government could be sued because they knew that the cheaper version of the MMR vaccine from the Urabe strain had a high risk of infection of AM(Aseptic Meningitis), and since the UK government indemnified vaccine manufacturers against lawsuits brought by possible damages from the MMR Urabe strain vaccine. This put the government of the UK in the crosshairs, and they couldn't have that, so they made Wakefield the scapegoat.
This is why the UK government officials, vaccine manufacturers and their thugs went against Wakefield so relentlessly.
It's conjecture as none of the subjects had aseptic meningitis and they were already in a legal case against the makers of the MMR vaccine.
The Urabe issue has been added to lend credence to Wakefield a long time after the case was decided..
And they went against Wakefield so relentlessly because he was a fraud.
A fraud who abused disabled children.
originally posted by: Pardon?
It's conjecture as none of the subjects had aseptic meningitis and they were already in a legal case against the makers of the MMR vaccine.
The Urabe issue has been added to lend credence to Wakefield a long time after the case was decided..
And they went against Wakefield so relentlessly because he was a fraud.
A fraud who abused disabled children.
It's not conjecture. The UK government gave the green light to use the cheaper version of the MMR vaccine containing the Urabe strain from 1988-1992, at the time that at least half of the children from the Lancet study were of age to receive this vaccine. The 1998 study did not find signs of aseptic meningitis because with time these children had been seeing regular doctors over the years, and they could have been very well treated with antivirals, or antibiotics (which will not cure it but will help treat the bacterial meningitis), or antifungals. Remember that many of these children had intestine problems as well, and they had been treated for years by other doctors which could have believed the children symptoms were caused by a virus.
Mumps and Measles are among the viruses that can cause aseptic meningitis, alongside influenza viruses, herpes viruses, arboviruses, or LCM (Lymphocytic choriomeningitis).
In case you didn't know aseptic meningitis can even be cured on it's own with time as well, but there are cases in which it leaves after effects that can be permanent.
Aseptic Meningitis
Written by Marissa Selner | Published on August 7, 2012
Medically Reviewed by Brenda B. Spriggs, MD, MPH, FACP on August 7, 2012
...
Treatment options depend on the specific cause of your meningitis. Many cases of viral meningitis are cured on their own within one to two weeks. You will be instructed to rest, stay hydrated, and use over-the-counter medications. Analgesics and/or anti-inflammatory medications may be recommended for pain and fever control.
...
Recovery and Long-Term Outlook
Less than 1 percent of patients with aseptic meningitis end up with a lasting illness. The majority of cases resolve within one to two weeks after the onset of symptoms.
In very rare cases, aseptic meningitis can lead to brain infections. Complications are more likely to occur if you do not seek treatment for your condition, or if you have an underlying condition that weakens your immune system.
...
www.healthline.com...
Other after effects that people can have even after aseptic meningitis has been cured.
After effects
Most people who get meningitis and septicaemia survive, often without any after effects, but sometimes these diseases cause a range of disabilities and problems that can alter people's lives.
After effects may be temporary or permanent, physical or emotional.
Relatives and friends may also feel the need for information, because the person who is recovering often needs a great deal of support.
Getting over meningitis or septicaemia can make major demands on people. Fortunately, many problems improve and disappear over time.
After effects of meningitis
Memory loss / difficulty retaining information / lack of concentration
Clumsiness / co-ordination problems
Residual headaches
Deafness / hearing problems / tinnitus / dizziness, loss of balance
Learning difficulties (ranging from temporary learning deficiencies to long term mental impairment)
Epilepsy / seizures (fits)
Weakness, paralysis or spasms of part of body (if permanent, sometimes called cerebral palsy)
Speech problems
Loss of sight/changes in sight
www.meningitis.org...
Is it out of the question that at least some of the children had aseptic meningitis? How can you say it is out of the question, when it is a known fact that the Urab strain of the MMR vaccine used in the UK from 1988-1992 were very probably used in some of the children from the Lancet 12 study, and these children had symptoms similar to the after effects of aseptic meningitis?
Aseptic meningitis can cause inflammation of the lining of the brain, and the underlying symptoms that can cause the inflammation of the brain can also cause intestinal illness.
...
Most viral meningitis is due to enteroviruses, which are viruses that also can cause intestinal illness.
Many other types of viruses can cause meningitis.
Viral meningitis can be caused by herpes viruses, the same virus that can cause cold sores and genital herpes . However, people with cold sores or genital herpes are not at a greater risk of developing herpes meningitis.
Viruses that cause mumps and HIV can cause aseptic meningitis.
Recently, West Nile virus, spread by mosquito bites, has become a cause of viral meningitis in most of the United States.
...
www.nlm.nih.gov...
The children could very well have been cured of the meningitis, but still have permanent effects that impaired them.
edit on 6-3-2015 by ElectricUniverse because: correct errors and add comment.
originally posted by: Pardon?
They're technicalities which weren't the crux of the case and just added to his overall sanctions.
I find it very convenient when you want to continuously ignore and dismiss the conflict of interests of the GMC hearing council because they were tied with vaccine manufacturing companies which had provided the vaccines used in these children among others. Not to mention that many of those involved did not declare this conflict of interest.
We know as a matter of fact that Dr. Horton was LYING because he is not an idiot. If he and the admins of the Free Royal saw the check, which they would have seen it, it would have shown that Dawbarns and litigators were paying the bill.
Then we have the fact that even Brian Deer did not disclose as to who was paying him. During the 160 day hearings the Sunday Times were not paying him to attend the hearings. So someone else must have been paying him. Not to mention the many LIES he was caught in.
The investigation into Wakefield had been one of the most intensive in over 50 years on any doctor.
Even in the book, MMR Science and Fiction: Exploring the Vaccine Crisis, which Dr. Horton authored he explained how health authorities had no idea where to begin, or how to resolve the "confusion".
‘…Indeed, the GMC seemed non-plussed by Reid's intervention. The best their spokeswoman could say was: 'We are concerned by these allegations and will be looking at what action, if any, may be necessary.' In truth, they had not a clue where to begin. At a dinner I attended on 23 February, one medical regulator and I discussed the Wakefield case. He seemed unsure of how the Council could play a useful part in resolving the confusion. As we talked over coffee while the other dinner guests were departing, he scribbled down some possible lines of investigation, and passed me his card, suggesting that I contact him directly if anything sprang to mind. He seemed keen to pursue Wakefield, especially given ministerial interest. Here was professionally led regulation of doctors in action - notes exchanged over liqueurs in a beautifully wood-panelled room of one of medicine's most venerable institutions…’ (Horton p.7-8) (1)
...
www.whale.to...
A very interesting fact is that Dr. Horton was editor-in-chief of the Lancet. The same newspaper which had many links to MMR vaccine manufacturers, including Sir Crispin Davis, who was appointed a non-executive director of drugs multinational Glaxo Smith Kline in 2003, and who was an editor of the Lancet, and the line editor of Brian Deer, the independent journalist who also made many false claims about himself and lied.
Heck, there were other facts that surfaced relating to one editor of the Lancet, and his brother, a judge who had rejected an appeal by MMR vaccine litigants.
...
Sir Nigel Davis was the judge who, three years ago, rejected an appeal by MMR vaccine litigants against the decision not to award funding for their legal campaign.
But he failed to mention his interests in the subject.
Now, complaints against him are being filed to the Office for Judicial Complaints, which investigates allegations of any questionable conduct by judges, coroners and magistrates.
Davis's brother, Sir Crispin Davis, was appointed a non-executive director of drugs multinational Glaxo Smith Kline in 2003, a year before the appeal came to court. Asked why Sir Nigel did not declare this, his spokesman said: "The possibility of any conflict of interest arising from his brother's position did not occur to him."
But Sir Crispin's potential links with MMR vaccines goes back longer than that, as since 1999 he had been CEO of Reed Elsevier, the publishing company which owns The Lancet magazine.
...
www.tmcnet.com...
originally posted by: Pardon?
The main points were that Wakefield HIMSELF did not declare any monies paid to him in respect of the legal case on submission of the study.
That is proven.
Already proved that is false. There is no way that Horton, and the admin at Royal Free didn't know when the check that was at the trustee fund at the Free Royal was signed by the Dawbarn lawyers. Not to mention that for a long time Barr, one of the Dawbarn lawyers, had been exchanging emails with Dr. Horton, and Barr had mentioned that Wakefield was going to work with them.
Here you go.
www.whale.to...
But Dr. Horton claimed he didn't know.
...
Richard Horton
False Testimony Before the GMC Richard Horton has been Editor of the UK Lancet since 1995. As editor, he has overall responsibility for everything that is published in the Lancet. He was well aware of Wakefield’s involvement in the MMR litigation a year before publication of the Lancet Case Series. Although Horton insisted that several measures be taken during editorial review to guard against misinterpretation of the findings reported in the limited case series, he found it unnecessary to require disclosure of Wakefield’s participation in the MMR litigation, which was widely known by the public and to vaccine regulators, at the end of the Lancet Case Series as a possible conflict of interest.
He was reminded again of the Wakefield-MMR litigation connection in a letter titled “litigation bias” (Rouse letter) sent just two working days after publication of the Case Series. Ex. 15. Dr. Horton published the Rouse letter and Dr. Wakefield’s reply but deleted Rouse’s reference to “litigation bias” and Rouse’s “black box” rendition of Wakefield’s participation in the MMR litigation. The deletion of the critical details of Wakefield’s involvement in the MMR litigation before publishing the Rouse letter in the Lancet enabled Horton to conceal his and the Lancet’s prior knowledge of these facts. Ex.
When Brian Deer made his allegations against Dr. Wakefield in 2004, Horton feigned ignorance, claiming that he first learned of Wakefield’s “prospective” involvement in the MMR litigation from Dr. Wakefield’s response to the Rouse letter published in the Lancet on May 2, 1998 (Ex. 16). Added to this clear evidence of abuse of his position both as an editor and a registered medical practitioner, Dr. Horton has publicly taken credit for engineering the GMC proceedings against Dr. Wakefield, Professor Murch, and Professor Walker-Smith.
He gave false testimony to GMC investigators and at the FTP hearing concerning his prior knowledge of Wakefield’s participation in the MMR litigation.
Dr. Horton’s Knowledge of Wakefield’s Participation in the MMR Litigation Prior to Publication of the Lancet Case Series.
Dr. B. D. Edwards, an employee of the Medicines Control Agency (MCA)wrote to the Lancet in March, 1997, complaining that text and tables from various Lancet papers had been reproduced in a Dawbarns Fact Sheet of March,
1997. Dawbarns prepared the Fact Sheet for its clients and other interested parties.
The Society for the Autistically Handicapped obtained a copy and posted it on the web. That Fact Sheet publicly disclosed Dawbarns’working relationship with Dr. Wakefield in the text accompanying the reference to Dr. Wakefield’s paper in The Lancet:
...
www.rescuepost.com...
(continued)
www.rescuepost.com...
You, alongside some others, want to claim that Wakefield was the fraud. You keep claiming there is no evidence to corroborate Wakefield's findings, when in this same thread research paper after research paper, and other evidence has been presented which refutes your claims and those of Dr. Horton, Brian Deer, et al.
You claimed that "any parent convinced would keep believing Wakefield", but you keep choosing to ignore the clear "conflict of interest" of Dr. Horton, Brian Deer, et al, and instead you want to claim that the parents are blind when they know more facts about this and what happened to their children that you can't phantom.
You have gone so far as clamining that parent 10 must have had interest in making money for drafting the Transfer Factor... It doesn't even occur you that his interest has been to help his child... Not to mention that the Transfer Factor wasn't done by Wakefield alone, other doctors were also involved in the patent.
In fact, if the parents believed the charges against Wakefield, they would be among the first to denounce him, yet they didn't. The accusations against Wakefield started with Brian Deer, who has been found to be lying time and again, and who hasn't declared who has been paying him because he only worked on "occasion" for the Lancet.
Not to mention the fact that in the patent the hospital Royal Free was named as the applicant. So it belonged to Royal Free, even though various doctors, including Wakefield were involved in the research of this patent... Even in Brian Deer's website you can see that it clearly says the applicant for the patent is the "Royal Free Hospital school of Medicine and Neuroimmuno Therapeutics Research Foundation."
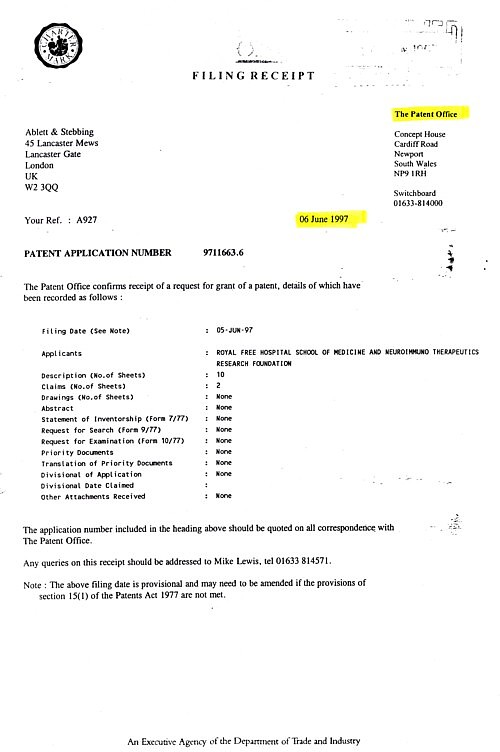
Wakefield then requested permission with the help of parent # 10 from the Free Royal to see if Transfer Factor could be used to help the children.
Then there is the fact that Brian Deer has made similar wrongful accusations of Dr. David Lewis which Deer completely made up.
www.rescuepost.com...
And
niceguidelines.files.wordpress.com...
The one who has been making false claims and has been a fraud from the start is Brian Deer, alongside Dr. Horton, and a few others who really had a conflict of interest.
www.rescuepost.com...
...
Richard Barr faxed a letter to Richard Horton at the Lancet on April 3, 1997. Ex. 3. Richard Barr’s letter and enclosures to Horton explained that Dawbarns was involved in litigation relating to damage to children caused by the MMR and MR vaccines, that he was working with Wakefield, that Wakefield had given permission to quote his Lancet papers in the Fact Sheet, that MCA and the Department of Health were pressuring the Lancet to have the references removed from the Fact Sheet, and that the Fact Sheet and correspondence from Dr. Susan Wood of the MCA would be sent by mail. The enclosed Fact Sheet was quite explicit about Wakefield’s involvement. He asked Richard Horton for retrospective permission to quote specific Lancet references “ contained in the fact sheet” and he identified the four relevant references by providing their footnote numbers in his letter. Footnote No. 50 on page 21 of the Fact Sheet was a reference to a paper co-authored by Wakefield. The text associated with that footnote reads
as follows:
There is convincing evidence of a link between vaccination and inflammatory bowel disease (including Crohn’s disease). It is a serious lifelong illness that has affected a large number of the children we are helping. We are working with Dr Andrew Wakefield of the Royal Free Hospital London. He is investigating this condition.
Exhibit 4 (emphasis added).
...
www.rescuepost.com...
You, alongside some others, want to claim that Wakefield was the fraud. You keep claiming there is no evidence to corroborate Wakefield's findings, when in this same thread research paper after research paper, and other evidence has been presented which refutes your claims and those of Dr. Horton, Brian Deer, et al.
You claimed that "any parent convinced would keep believing Wakefield", but you keep choosing to ignore the clear "conflict of interest" of Dr. Horton, Brian Deer, et al, and instead you want to claim that the parents are blind when they know more facts about this and what happened to their children that you can't phantom.
You have gone so far as clamining that parent 10 must have had interest in making money for drafting the Transfer Factor... It doesn't even occur you that his interest has been to help his child... Not to mention that the Transfer Factor wasn't done by Wakefield alone, other doctors were also involved in the patent.
In fact, if the parents believed the charges against Wakefield, they would be among the first to denounce him, yet they didn't. The accusations against Wakefield started with Brian Deer, who has been found to be lying time and again, and who hasn't declared who has been paying him because he only worked on "occasion" for the Lancet.
Not to mention the fact that in the patent the hospital Royal Free was named as the applicant. So it belonged to Royal Free, even though various doctors, including Wakefield were involved in the research of this patent... Even in Brian Deer's website you can see that it clearly says the applicant for the patent is the "Royal Free Hospital school of Medicine and Neuroimmuno Therapeutics Research Foundation."
Wakefield then requested permission with the help of parent # 10 from the Free Royal to see if Transfer Factor could be used to help the children.
Then there is the fact that Brian Deer has made similar wrongful accusations of Dr. David Lewis which Deer completely made up.
November 13.2012
Joseph Gow. Chancellor
The Universitv of
Wisconsin-La Crosse
i 725 State St, 135 GMH
La Crosse, WI 5460 I
RE Brian Deer's comments concerning Dr. David Lewis
Dear Chancellor Gow
Brian Deer, as you may know, gave a series of lectures at the University of Wisconsin-La Crosse (UW-L) on October 4-5 concerning the 1998 !-llcel study published by Dr. Andrew Waketìeld and others at the University College London (L!CL)
According to an audiotape of one of Mr. Deer's lectures posted on the Internet, and postings he placed on his personal website, Mr. Deer appears to be using his UW-L lectures to defame Dr. David Lewis 1, whom I have represented for the past 16 years in a number of environmental whistleblower cases. Mr. Deer's attacks appear to be motivated by a report Dr. Lewis submitted to the UX Research Integrity Ot1ce (UKRIO) in 20 I I.
The report, which contained unpublished documents Dr. Lewis obtained from Dr. Wakefìeld's fìles, raise serious concerns about Deer's handling of the evidence he gathered during his reporting on the Lancet study.
Among the documents Dr. Lewis recovered was an expert report prepared in 2006 by one of the General Medical Council's (GMC's) witnesses, Professor Ian Booth. Surprisingly, it matches the analysis of patient records Deer published four years later as his own original work Booth's report is a perfect intellectual template for Deer's articles published in the RMJ. Perhaps most shocking of all, Dr. Lewis obtained a copy of a document showing that, in 2004, the UK. Freedom of Information ot1ce provided Mr. Deer copies of ethics approvals for the research component of the Lancet study, which he apparently never passed on to the GMC. A number of Mr. Deer's allegations of research misconduct rest upon the absence of any evidence that Dr. Wakefield and his coauthors ever obtained the necessary ethics approvals to cover the research component of the Lancet study.
Dr. Lewis's report also included copies of letters exchanged between Lancet editor Richard Horton and Attorney Richard Barr. Deer accuses Dr. Waketìeld of not disclosing his expert witness work for Mr. Barr to Lancet's editors. These letters predate publication of the rancel article by approximately nine months. Dr. Lewis's report also contained copies of many of the original biopsy grading sheets upon which the Lancet article was based, as well as photomicrographs of missing biopsy slides for most of the children who participated in the study. In one of his aricles published in the BMJ, Deer alleged that Dr. Wakefield used these grading sheets to fabricate the diagnosis of colitis reported for most of the children in the Lancel study.
...
www.rescuepost.com...
And
niceguidelines.files.wordpress.com...
The one who has been making false claims and has been a fraud from the start is Brian Deer, alongside Dr. Horton, and a few others who really had a conflict of interest.
...
According to an audiotape of Mr. Deer's presentation at UW-L on October 4, Mr. Deer said that Dr. Lewis was fired by the Environmental Protection Agency for, uh after, very serious allegations o.f misconduct. Similarly, on his personal website where he rebukes Jennifer VanDerHorst-Larson for speaking highly of Dr. Lewis, Deer repeats this fabrication, stating Dr. Lewis was fired by the Environmental Protection Agency in 2003 following unresolved allegations of research misconduct.
...
www.rescuepost.com...
new topics
-
Las Vegas UFO Spotting Teen Traumatized by Demon Creature in Backyard
Aliens and UFOs: 2 hours ago -
2024 Pigeon Forge Rod Run - On the Strip (Video made for you)
Automotive Discussion: 3 hours ago -
Gaza Terrorists Attack US Humanitarian Pier During Construction
Middle East Issues: 3 hours ago -
The functionality of boldening and italics is clunky and no post char limit warning?
ATS Freshman's Forum: 4 hours ago -
Meadows, Giuliani Among 11 Indicted in Arizona in Latest 2020 Election Subversion Case
Mainstream News: 5 hours ago -
Massachusetts Drag Queen Leads Young Kids in Free Palestine Chant
Social Issues and Civil Unrest: 5 hours ago -
Weinstein's conviction overturned
Mainstream News: 6 hours ago -
Supreme Court Oral Arguments 4.25.2024 - Are PRESIDENTS IMMUNE From Later Being Prosecuted.
Above Politics: 8 hours ago -
Krystalnacht on today's most elite Universities?
Social Issues and Civil Unrest: 8 hours ago -
Chris Christie Wishes Death Upon Trump and Ramaswamy
Politicians & People: 8 hours ago
top topics
-
Krystalnacht on today's most elite Universities?
Social Issues and Civil Unrest: 8 hours ago, 9 flags -
Weinstein's conviction overturned
Mainstream News: 6 hours ago, 7 flags -
Supreme Court Oral Arguments 4.25.2024 - Are PRESIDENTS IMMUNE From Later Being Prosecuted.
Above Politics: 8 hours ago, 7 flags -
University of Texas Instantly Shuts Down Anti Israel Protests
Education and Media: 11 hours ago, 6 flags -
Massachusetts Drag Queen Leads Young Kids in Free Palestine Chant
Social Issues and Civil Unrest: 5 hours ago, 4 flags -
Meadows, Giuliani Among 11 Indicted in Arizona in Latest 2020 Election Subversion Case
Mainstream News: 5 hours ago, 4 flags -
Gaza Terrorists Attack US Humanitarian Pier During Construction
Middle East Issues: 3 hours ago, 3 flags -
Chris Christie Wishes Death Upon Trump and Ramaswamy
Politicians & People: 8 hours ago, 2 flags -
Any one suspicious of fever promotions events, major investor Goldman Sachs card only.
The Gray Area: 13 hours ago, 2 flags -
2024 Pigeon Forge Rod Run - On the Strip (Video made for you)
Automotive Discussion: 3 hours ago, 1 flags
active topics
-
Meadows, Giuliani Among 11 Indicted in Arizona in Latest 2020 Election Subversion Case
Mainstream News • 10 • : chr0naut -
Supreme Court Oral Arguments 4.25.2024 - Are PRESIDENTS IMMUNE From Later Being Prosecuted.
Above Politics • 75 • : Vermilion -
University student disciplined after saying veganism is wrong and gender fluidity is stupid
Education and Media • 50 • : watchitburn -
VP's Secret Service agent brawls with other agents at Andrews
Mainstream News • 55 • : CarlLaFong -
Cats Used as Live Bait to Train Ferocious Pitbulls in Illegal NYC Dogfighting
Social Issues and Civil Unrest • 23 • : Ravenwatcher -
-@TH3WH17ERABB17- -Q- ---TIME TO SHOW THE WORLD--- -Part- --44--
Dissecting Disinformation • 680 • : 777Vader -
Is there a hole at the North Pole?
ATS Skunk Works • 40 • : Oldcarpy2 -
Fossils in Greece Suggest Human Ancestors Evolved in Europe, Not Africa
Origins and Creationism • 89 • : whereislogic -
University of Texas Instantly Shuts Down Anti Israel Protests
Education and Media • 197 • : NorthOS -
Candidate TRUMP Now Has Crazy Judge JUAN MERCHAN After Him - The Stormy Daniels Hush-Money Case.
Political Conspiracies • 790 • : Oldcarpy2